Essential Components of the Immune System - Innate and Adaptive Immunity and the Chronological Immune Response to Viral Infections
Table of Contents
- The Immune System as a Health Resource
- Structure of the Immune System: Innate and Adaptive System
- The First Line of Defense — The Non-Specific Immune System
- Phases of the Immune Response — From Innate to Adaptive Immunity
- Dendritic Cells — Key Cells of the Adaptive Immune Response
- Natural Killer Cells (NK Cells) — Early Cellular Defense
- Innate Lymphoid Cells (ILCs) — Relatives of NK Cells
- Specific Immunity — The Role of Lymphocytes
- Immune Cells Between Standby Mode and Highly Active Killer Status
- Chronological Immune Response to Viral Infections
- Self-Regulation — The Organism’s Self-Protection
- Subjective Symptoms and Laboratory Diagnostics
- References
- One-Minute-Paper Topics
1 The Immune System as a Health Resource
From a physical perspective, the immune system represents a central health resource. It depends on the integrity of the body’s barrier surfaces (skin, mucous membranes), adequate cell functions, and sufficient mobility of immune cells within the organism. The immune system develops across the lifespan and is closely linked to the musculoskeletal system — muscle mass and immune functions decline with age. The autonomic nervous system has a decisive connection to the immune system: the sympathetic nervous system has proinflammatory effects, while the parasympathetic nervous system has anti-inflammatory effects. Physical exertion shapes the immune system both acutely (short-term) and chronically (long-term). Dysfunctions manifest as infections, atherosclerosis, cancer, allergies, and autoimmune diseases (Puta et al. 2026).
2 Structure of the Immune System: Innate and Adaptive System
In vertebrates, the immune system consists of a finely regulated system of molecules, proteins, and processes with two main components: the innate and the adaptive immune system.
General tasks of the immune system include: host-microorganism interaction, cellular and intercellular efficacy, initiation and termination of cellular life, as well as balance and equilibrium of immune functions.
Properties and functions include: antigen binding, phagocytosis and antigen processing, antigen presentation, cell activation and proliferation, cellular and antibody-mediated immune responses, intercellular communication, diversity, specificity, memory, and self/non-self discrimination (Puta et al. 2026; Rich et al. 2012).
3 The First Line of Defense — The Non-Specific Immune System
The body’s defense is organized in multiple staggered levels. The barrier surfaces of the organism are of particular importance: skin, mucous membranes, and tear fluid form a first barrier against foreign bodies and pathogens. Mucous membranes are found in the airways, the oral, nasal, and pharyngeal cavities, the bronchi, the lungs, the entire digestive tract, and the urinary tract.
When this barrier layer is breached, the next defense levels come into action. Neutrophil granulocytes (phagocytes) engulf and destroy the pathogen. Macrophages transport pathogens to the nearest lymph node and function as antigen-presenting cells (Puta et al. 2026; Baumann and Gauldie 1994).
4 Phases of the Immune Response — From Innate to Adaptive Immunity
The cellular immune response is triggered when sensor cells (macrophages, neutrophils, dendritic cells) detect so-called inflammatory inducers. These inducers include molecular structures indicating the presence of pathogens or tissue damage — for example, bacterial lipopolysaccharides, ATP, or urate crystals. Recognition occurs via innate pattern recognition receptors (PRRs), which are encoded by a limited number of genes and remain constant throughout the lifespan (Murphy and Weaver 2016).
Activation of sensor cells leads to the production of various mediators, particularly cytokines, which either directly contribute to the destruction of invading pathogens or act on other cells to amplify the immune response. The immune response proceeds in characteristic phases with distinct temporal dynamics (Murphy and Weaver 2016):
Temporal dynamics of the immune response, from innate onset to lasting memory.
| Phase | Onset After Infection | Duration |
|---|---|---|
| Inflammation, complement activation, phagocytosis (innate) | Minutes | Days |
| Dendritic cell–T cell interaction: antigen recognition, adhesion, co-stimulation, T cell proliferation | Hours | Days |
| Activation of antigen-specific B cells | Hours | Days |
| Formation of effector and memory T cells | Days | Weeks |
| T cell–B cell interaction, germinal center formation, antibody production | Days | Weeks |
| Emigration of effector lymphocytes from peripheral lymphoid organs | A few days | Weeks |
| Elimination of pathogen by effector cells and antibodies | A few days | Weeks |
| Immunological memory: maintenance of memory B and T cells | Days to weeks | Can be lifelong |
Temporal dynamics of the immune response, from innate onset to lasting memory.
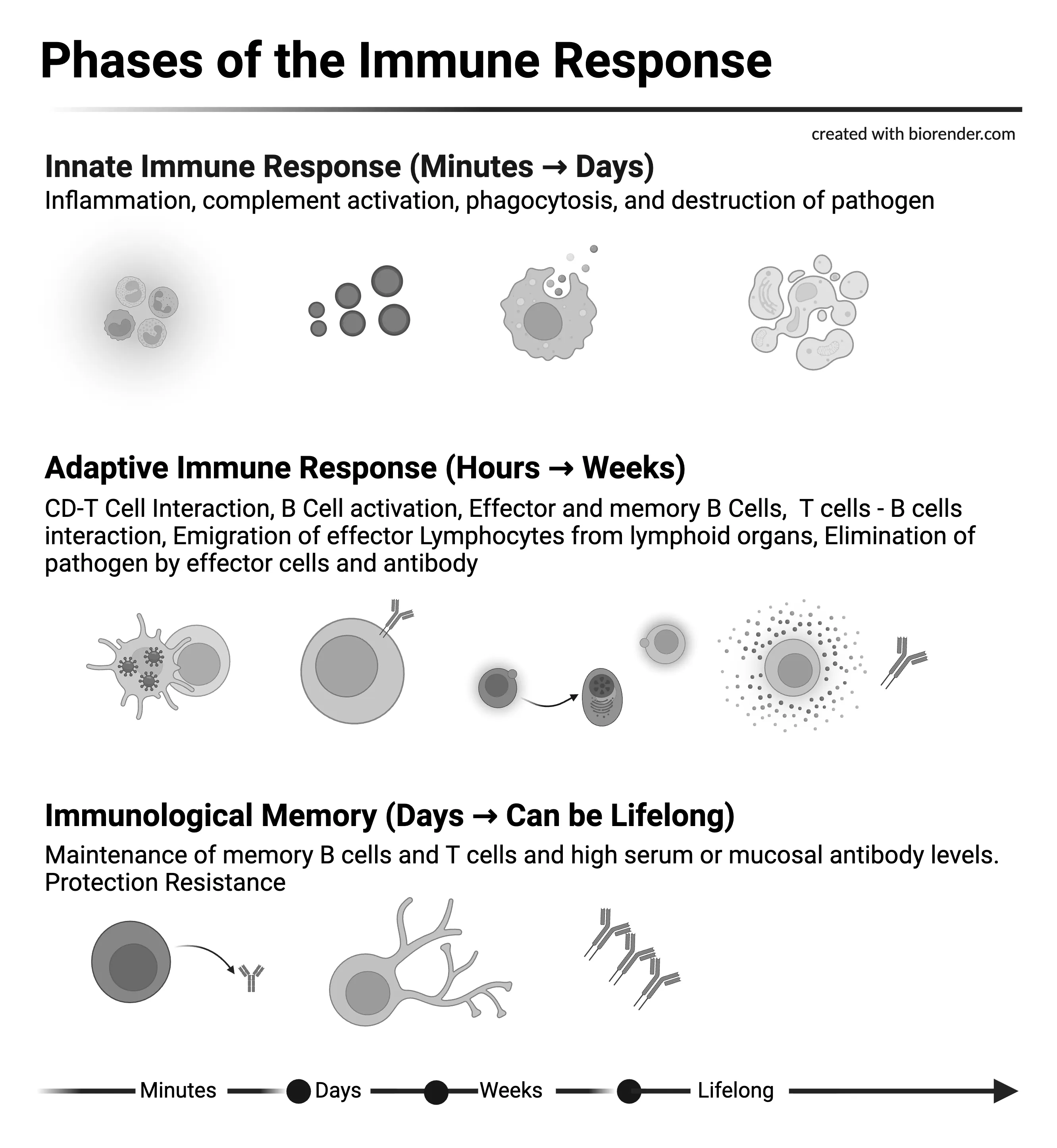
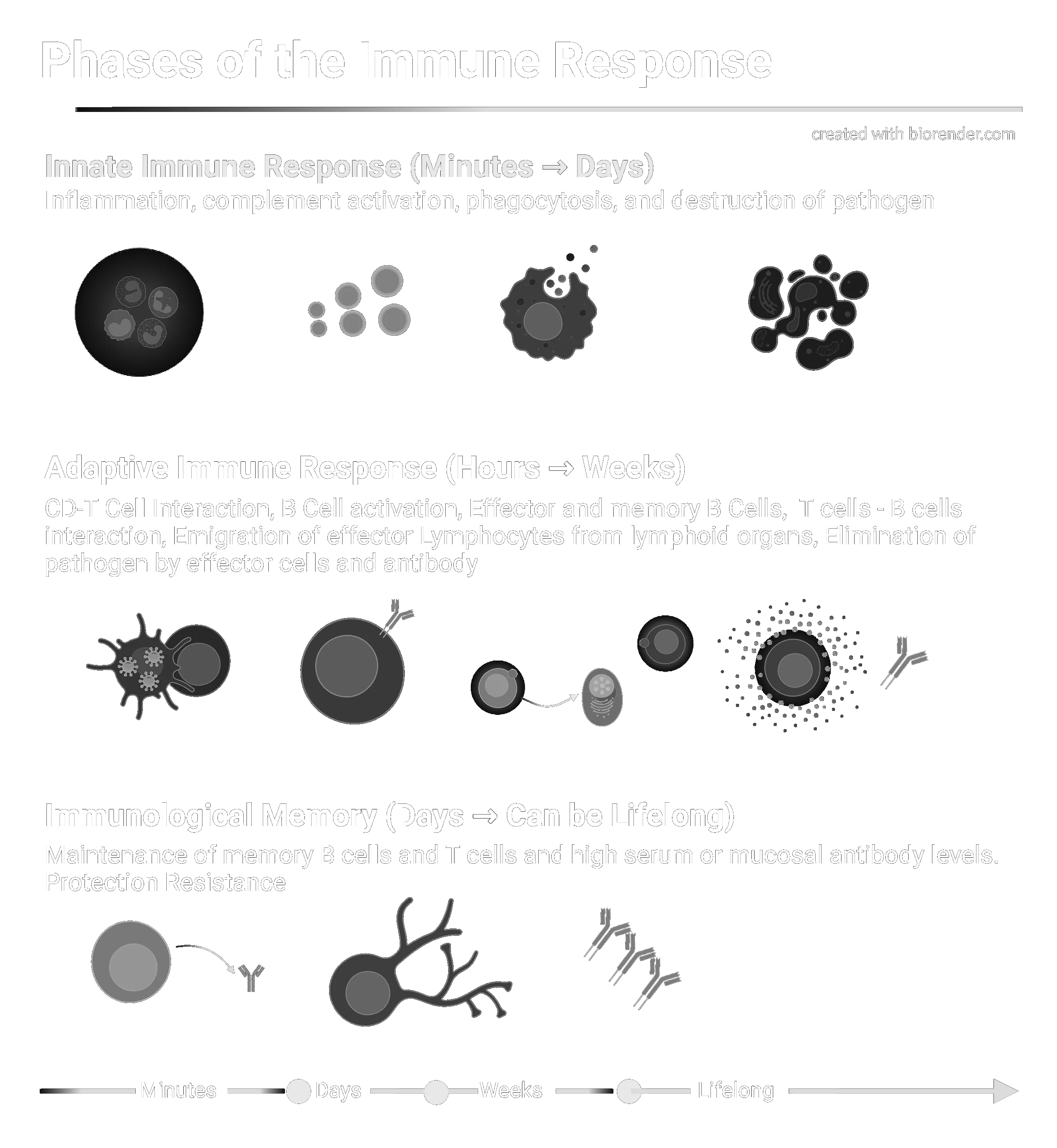
This phase overview illustrates that the innate immune response reacts within minutes, while the adaptive immune response requires days to fully develop. Crucially, the adaptive immune response can eliminate infections far more efficiently than the innate immune response alone due to its exquisite specificity (Murphy and Weaver 2016).
Phases of the Immune Response — Gantt-Style Timeline Chart. The innate immune response (black) is initiated within minutes; the adaptive response (dark grey) develops over days to weeks; immunological memory (medium grey, dotted) can persist lifelong. Onset dots mark the beginning of each phase. Adapted from Murphy K & Weaver C (2016). Janeway’s Immunobiology, 9th edn.
Phases of the Immune Response — Gantt-Style Timeline Chart. The innate immune response (black) is initiated within minutes; the adaptive response (dark grey) develops over days to weeks; immunological memory (medium grey, dotted) can persist lifelong. Onset dots mark the beginning of each phase. Adapted from Murphy K & Weaver C (2016). Janeway’s Immunobiology, 9th edn.
5 Dendritic Cells — Key Cells of the Adaptive Immune Response
Dendritic cells serve a central bridging function between the innate and adaptive immune systems. In their immature state, they reside in peripheral tissues where they take up pathogens and their antigens through macropinocytosis and receptor-mediated endocytosis (Murphy and Weaver 2016).
Recognition of pathogen-associated molecular patterns (PAMPs) by PRRs stimulates dendritic cells to migrate via lymphatic vessels to regional lymph nodes. During this migration, the cells undergo a maturation process: they lose their phagocytic capacity but instead present peptide antigens on their MHC molecules and express co-stimulatory molecules essential for the complete activation of naive T cells (Murphy and Weaver 2016).
As antigen-presenting cells (APCs), mature dendritic cells stimulate the proliferation and differentiation of T lymphocytes in lymph nodes. The activation of naive T lymphocytes by dendritic cells thus represents an essential first step in virtually all adaptive immune responses. While macrophages and B cells can also function as APCs under certain circumstances, dendritic cells are the specialized initiators of adaptive immunity (Murphy and Weaver 2016; Puta et al. 2026).
Dendritic cells initiate adaptive immune responses. Immature dendritic cells in peripheral tissue take up pathogens via macropinocytosis and receptor-mediated endocytosis, then migrate to regional lymph nodes where they mature and activate naive T cells via antigen presentation and co-stimulatory molecules. Adapted from Murphy K & Weaver C (2016). Janeway’s Immunobiology, 9th edn.
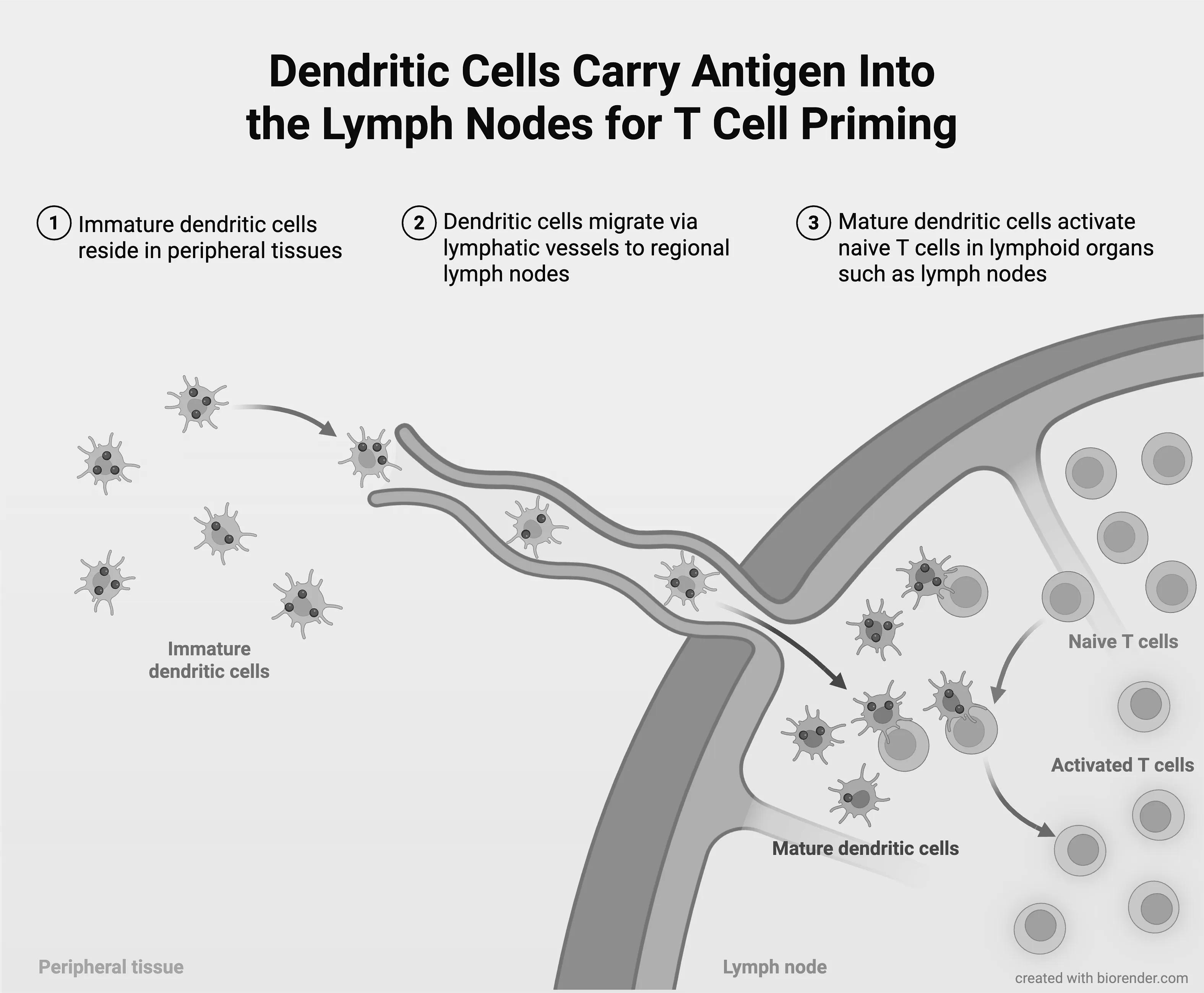
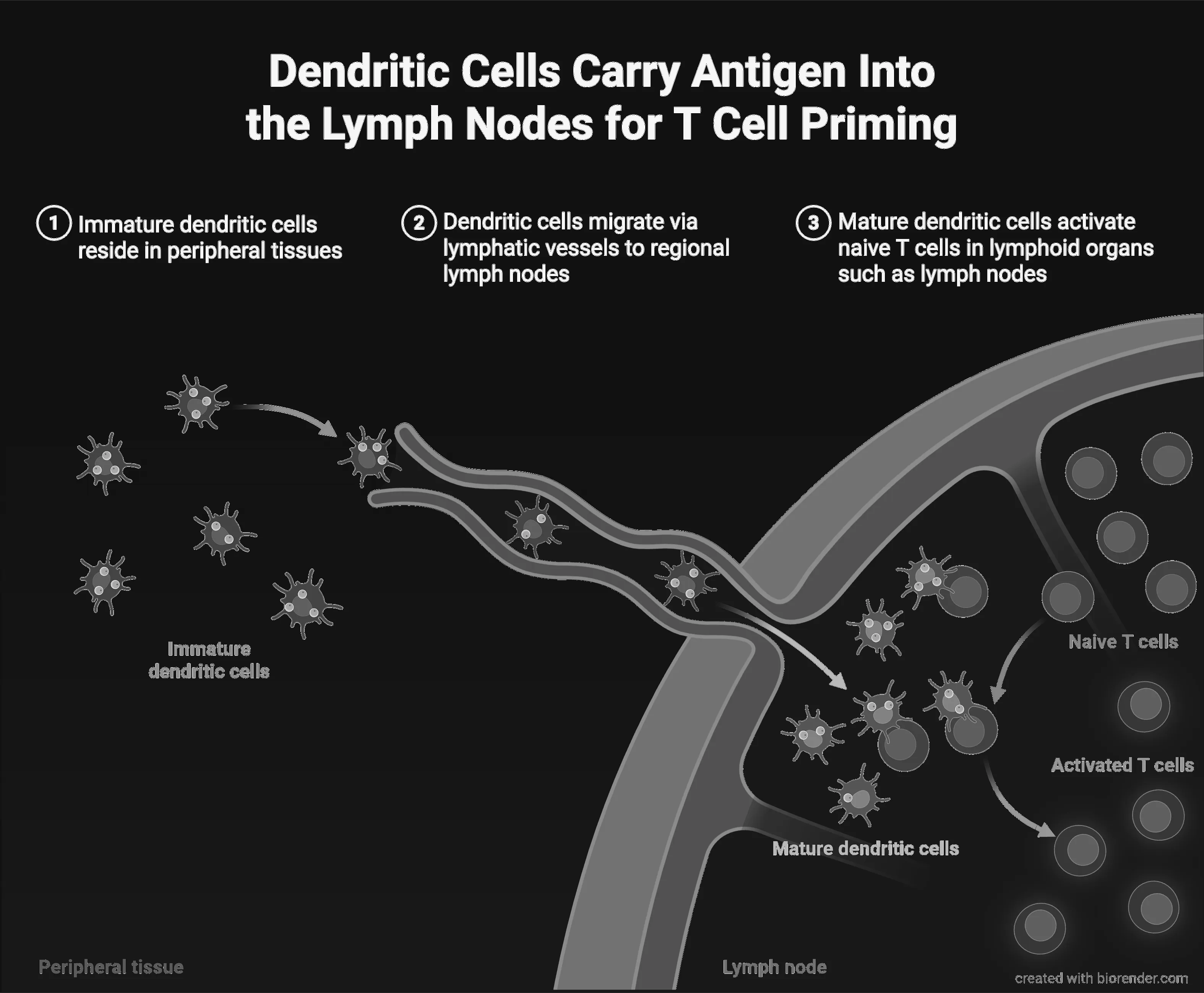
Dendritic cells initiate adaptive immune responses. Immature dendritic cells in peripheral tissue take up pathogens via macropinocytosis and receptor-mediated endocytosis, then migrate to regional lymph nodes where they mature and activate naive T cells via antigen presentation and co-stimulatory molecules. Adapted from Murphy K & Weaver C (2016). Janeway’s Immunobiology, 9th edn.
6 Natural Killer Cells (NK Cells) — Early Cellular Defense
NK cells are lymphocytes of the innate immune system that are larger than T and B cells and contain characteristic cytoplasmic granules with cytotoxic proteins. They are functionally identified by their ability to kill certain tumor cell lines in vitro without requiring prior specific immunization (Murphy and Weaver 2016).
6.1 Activation Mechanisms
NK cells are activated by type I interferons (IFN-α, IFN-β) as well as cytokines produced by macrophages, particularly IL-12 and TNF-α. IL-12 acts synergistically with IL-18 and stimulates NK cells to secrete large amounts of IFN-γ. This is crucial for controlling infections in the early phase before the adaptive immune response becomes available (Murphy and Weaver 2016).
6.2 Cytotoxic Mechanisms
NK cells kill target cells via two main mechanisms:
- Granule exocytosis: Release of granzymes and perforin from cytotoxic granules onto the surface of the target cell, leading to penetration of the cell membrane and induction of programmed cell death — a mechanism corresponding to that of cytotoxic T cells.
- TRAIL pathway: NK cells express the TNF family ligand TRAIL (Tumor Necrosis Factor-Related Apoptosis-Inducing Ligand), which interacts with death receptors DR4 and DR5 on target cells and triggers apoptosis.
6.3 Activating and Inhibitory Receptors
In contrast to T and B cells, NK cells use germline-encoded receptors to distinguish between healthy and infected or malignantly transformed cells. NK cells express both activating and inhibitory receptors. The integration of these signals determines whether a target cell is killed. Inhibitory receptors recognize MHC class I molecules on healthy cells, preventing their destruction. When infected or transformed cells downregulate their MHC-I expression, activating signals predominate and the target cell is eliminated (Murphy and Weaver 2016).
6.4 Role in Antiviral Defense
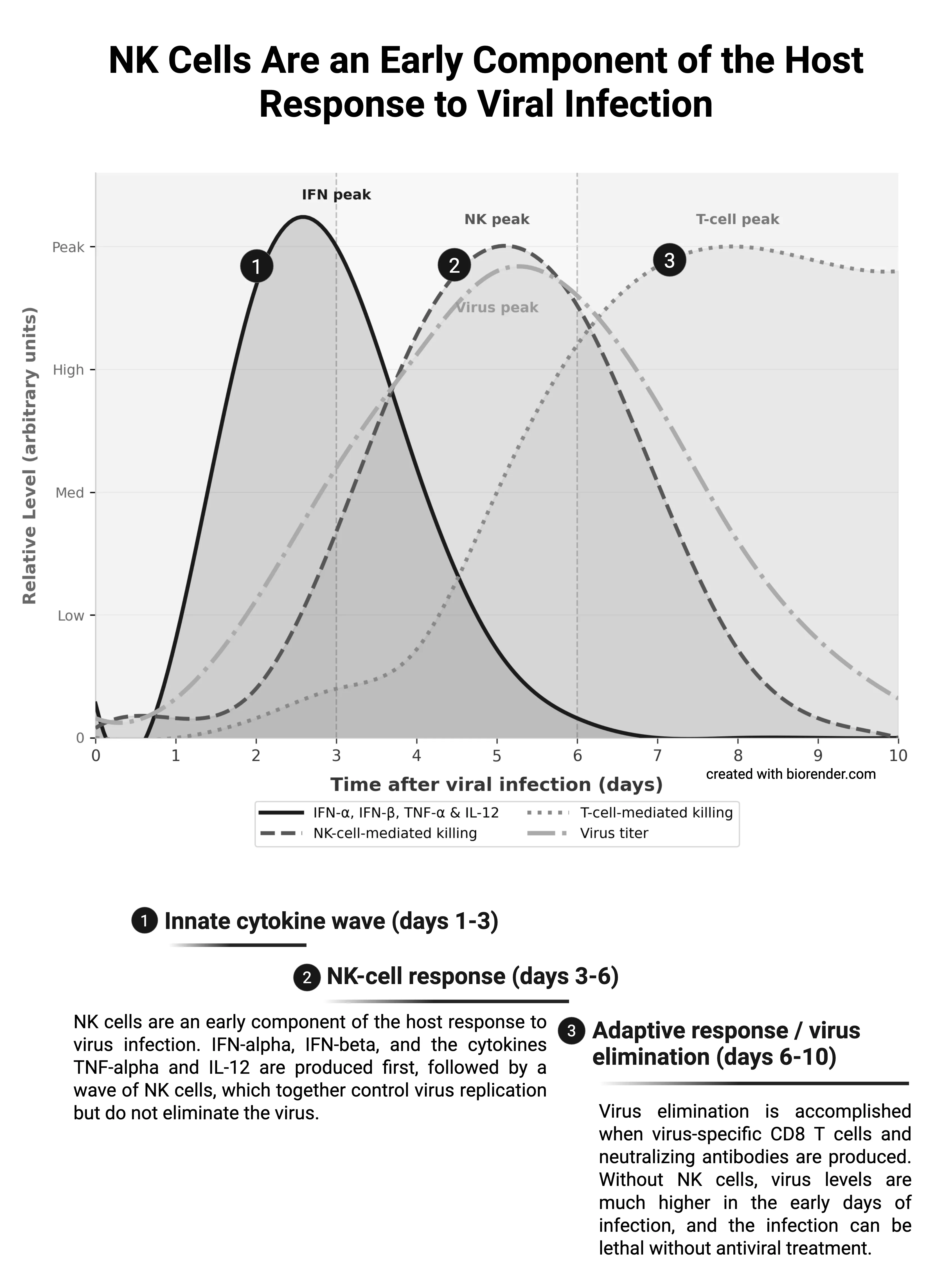
NK cells serve to contain viral infections while the adaptive immune system generates antigen-specific cytotoxic T cells and neutralizing antibodies. The temporal sequence of antiviral defense shows that IFN-α, IFN-β, TNF-α, and IL-12 are produced first, followed by a wave of NK cell activity that collectively controls virus replication without completely eliminating the virus. Final virus elimination is accomplished only by virus-specific CD8 T cells and neutralizing antibodies. The clinical relevance of NK cells is underscored by rare patients with selective NK cell deficiency who exhibit increased susceptibility to herpesvirus infections (Murphy and Weaver 2016).
Furthermore, NK cells produce TNF-α, GM-CSF, and the chemokines CCL3, CCL4, and CCL5 in addition to IFN-γ, contributing to the recruitment and activation of macrophages. IFN-γ from NK cells directly activates macrophages and influences the differentiation of CD4 T cells into the proinflammatory TH1 subset (Murphy and Weaver 2016).
NK cells are an early component of the host response to virus infection. IFN-α/IFN-β and cytokines (black, solid) are produced first, followed by NK-cell killing (dark grey, dashed); T-cell killing (medium grey, dotted) peaks later as the adaptive response matures. Virus titer (light grey, dash-dot) rises then falls once adaptive immunity is established. Adapted from Murphy K & Weaver C (2016). Janeway’s Immunobiology, 9th edn.
NK cells are an early component of the host response to virus infection. IFN-α/IFN-β and cytokines (black, solid) are produced first, followed by NK-cell killing (dark grey, dashed); T-cell killing (medium grey, dotted) peaks later as the adaptive response matures. Virus titer (light grey, dash-dot) rises then falls once adaptive immunity is established. Adapted from Murphy K & Weaver C (2016). Janeway’s Immunobiology, 9th edn.
7 Innate Lymphoid Cells (ILCs) — Relatives of NK Cells
In addition to NK cells, a family of innate lymphoid cells (ILCs) exists whose subtypes closely parallel the subpopulations of effector CD4 and CD8 T cells. ILC1, ILC2, and ILC3 cells differ in their cytokine profiles and functions (Murphy and Weaver 2016):
- ILC1: Produce IFN-γ; require the transcription factor Tbet and the cytokine IL-7.
- ILC2: Produce IL-4, IL-5, and IL-13 in response to TSLP and IL-33; promote mucosal and barrier immunity as well as defense against parasites.
- ILC3: Respond to IL-1β and IL-23; produce IL-17 and IL-22, which enhance defense mechanisms against extracellular bacteria and fungi.
NK cells themselves require the cytokine IL-15 and the transcription factors Nfil3 and eomesodermin for their development, distinguishing them from other ILC subtypes (Murphy and Weaver 2016).
8 Specific Immunity — The Role of Lymphocytes
The pathogen fragments presented by dendritic cells are recognized by lymphocytes. T helper cells recognize the presented antigens and regulate the further immune response. B lymphocytes and plasma cells produce specific immunoglobulins (antibodies), which can be produced in large quantities within a few days. The antigen-antibody complexes are phagocytosed and eliminated by phagocytes (Puta et al. 2026; Goldsby et al. 2003).
9 Immune Cells Between Standby Mode and Highly Active Killer Status
Normally, immune cells are in a largely inactive state. Through direct contact with pathogens, their toxins, or through cytokines from other immune cells, they are shifted to a highly active state (effector cells). A primary reason for activation is antigens, but also physical activity (Puta et al. 2026).
10 Chronological Immune Response to Viral Infections
The immune response to viral infections follows a clear temporal sequence that reflects the previously described phases of the immune response:
10.1 Immediate Response (Minutes to Hours)
Phagocytes (monocytes/macrophages, neutrophils) and natural killer cells are responsible for the non-specific immediate response. NK cells are activated by type I interferons and macrophage-derived cytokines and control virus replication in the early phase (Murphy and Weaver 2016). They release signaling molecules that attract other immune cells to the site of infection, induce inflammatory tissue changes (redness, swelling, pain), and in strong reactions activate the temperature regulation center in the brain (fever). Simultaneously, dendritic cells take up pathogens and begin their migration to lymph nodes, where they initiate the adaptive immune response (Murphy and Weaver 2016; Puta et al. 2026).
10.2 Adaptive Effector Response (2—10 Days)
Using SARS-CoV-2 as an example, the first specific helper T cells (CD4⁺) are detectable 2—4 days after symptom onset. This activation occurs in secondary lymphoid organs through interaction with mature dendritic cells that have migrated from the site of infection and present antigens on MHC molecules (Murphy and Weaver 2016). After 6—10 days, the number of adaptive effector cells has reached sufficient levels to control the viral infection. Viral load peaks on days 5—6, and approximately 90% of individuals seroconvert by day 10 (Sette and Crotty 2021; Puta et al. 2026).
10.3 Immunological Memory
Following viral elimination, T cells form memory T cell pools that peak within 2 weeks and are detectable for over 100 days. B cells transform into memory cells and long-lived plasma cells. This phase of immunological memory can persist lifelong and provides protection against reinfection (Hope and Bradley 2021; Murphy and Weaver 2016).
11 Self-Regulation — The Organism’s Self-Protection
To prevent the inflammatory response from overshooting, the organism self-regulates through anti-inflammatory signaling molecules and hormones (e.g., cortisol) as well as regulatory T cells. Stress hormones such as epinephrine and cortisol significantly alter the circulation patterns of immune cells and suppress immune function at persistently elevated levels (Puta et al. 2026; Cupps and Fauci 1982).
12 Subjective Symptoms and Laboratory Diagnostics
Signs of optimal immunity: Vitality, functional and physical performance capacity, adequate recovery ability, good wound healing, appropriate vaccination response, few infectious diseases per year.
Laboratory diagnostics in 3 levels:
- Level 1: Erythrocyte sedimentation rate, complete blood count, C-reactive protein, urinalysis
- Level 2: Monocyte subpopulations, T cell subpopulations, pathogen-specific immunoglobulins
- Level 3: In vitro functional tests, molecular biology tests, complement factors
References
- Baumann H, Gauldie J (1994) The acute phase response. Immunol Today 15(2):74-80.
- Cupps TR, Fauci AS (1982) Corticosteroid-mediated immunoregulation in man. Immunol Rev 65:133-155.
- Goldsby RA et al. (2003) Immunology, 5th edn. W.H. Freeman.
- Hope JL, Bradley LM (2021) Lessons in antiviral immunity. Science 371:464-465.
- Murphy K, Weaver C (2016) Janeway’s Immunobiology, 9th edn. Garland Science.
- Puta C, Haunhorst S, Gabriel HHW (2026) Sport und Immunsystem. In: Wonisch M et al. (eds) Kompendium der Sportmedizin. Springer.
- Rich RR et al. (2012) Clinical Immunology, 4th edn.
- Sette A, Crotty S (2021) Adaptive immunity to SARS-CoV-2 and COVID-19. Cell 184(4):861-880.
One-Minute-Paper Topics
A One-Minute-Paper (OMP) is a short, focused prompt that students answer in ~60 seconds at the end of a session to consolidate learning, surface misconceptions, and provide formative feedback. When answering, be concise, specific, and use terminology from today’s session.
- In one or two sentences, define the core functional difference between the innate and the adaptive immune system.
- Name three cellular components of the innate immune system and state one key function of each.
- Why is the dendritic cell often called the “bridge” between innate and adaptive immunity?
- Sketch (in words) the chronological sequence of immune events during the first 14 days after a viral infection.
- What distinguishes a Natural Killer (NK) cell from a cytotoxic CD8⁺ T cell in terms of target recognition?
- Explain in your own words what “antigen presentation” means and why MHC molecules are required.
- List the main lymphocyte subsets and assign each to either the innate or the adaptive arm.
- What is the biological purpose of the acute phase response, and which organ orchestrates it?
- Describe one situation in which the innate response alone is insufficient to clear a viral pathogen.
- Why does the adaptive immune response need several days before becoming effective?
- What is immunological memory, and which cell types carry it?
- Compare the three levels of complexity of immunological laboratory diagnostics introduced in the lecture.
- Which single laboratory parameter would you request first if you suspected an acute viral infection in an athlete, and why?
- Explain the difference between humoral and cell-mediated adaptive immunity using one example each.
- What was the most surprising or counter-intuitive fact you learned in today’s lecture?
- Which concept from today’s lecture do you still find unclear or confusing?
- How would you explain the role of cytokines to a fellow student in two sentences?
- Give one example of how a defect in the innate immune system could compromise adaptive responses.
- Why is the chronology of the antiviral immune response clinically relevant for interpreting blood tests?
- What is one question this lecture raised that you would like to explore further?