Teaching Anaerobic Threshold
Table of Contents
- Definition of the anaerobic threshold
- Worked example: determining the IAT after Stegmann et al. (1981)
- The anaerobic threshold as a metabolic, hormonal and immunological breakpoint
- Exercise prescription based on the anaerobic threshold
- Trained versus untrained subjects
- The anaerobic threshold and percentages of VO₂max / HRmax
- Strengths and weaknesses of the anaerobic-threshold concept
- 7.1 Strengths
- 7.2 Weaknesses
- Summary in one paragraph
- References
- One-Minute-Paper Topics
1. Definition of the anaerobic threshold
1.1 The aerobic–anaerobic transition
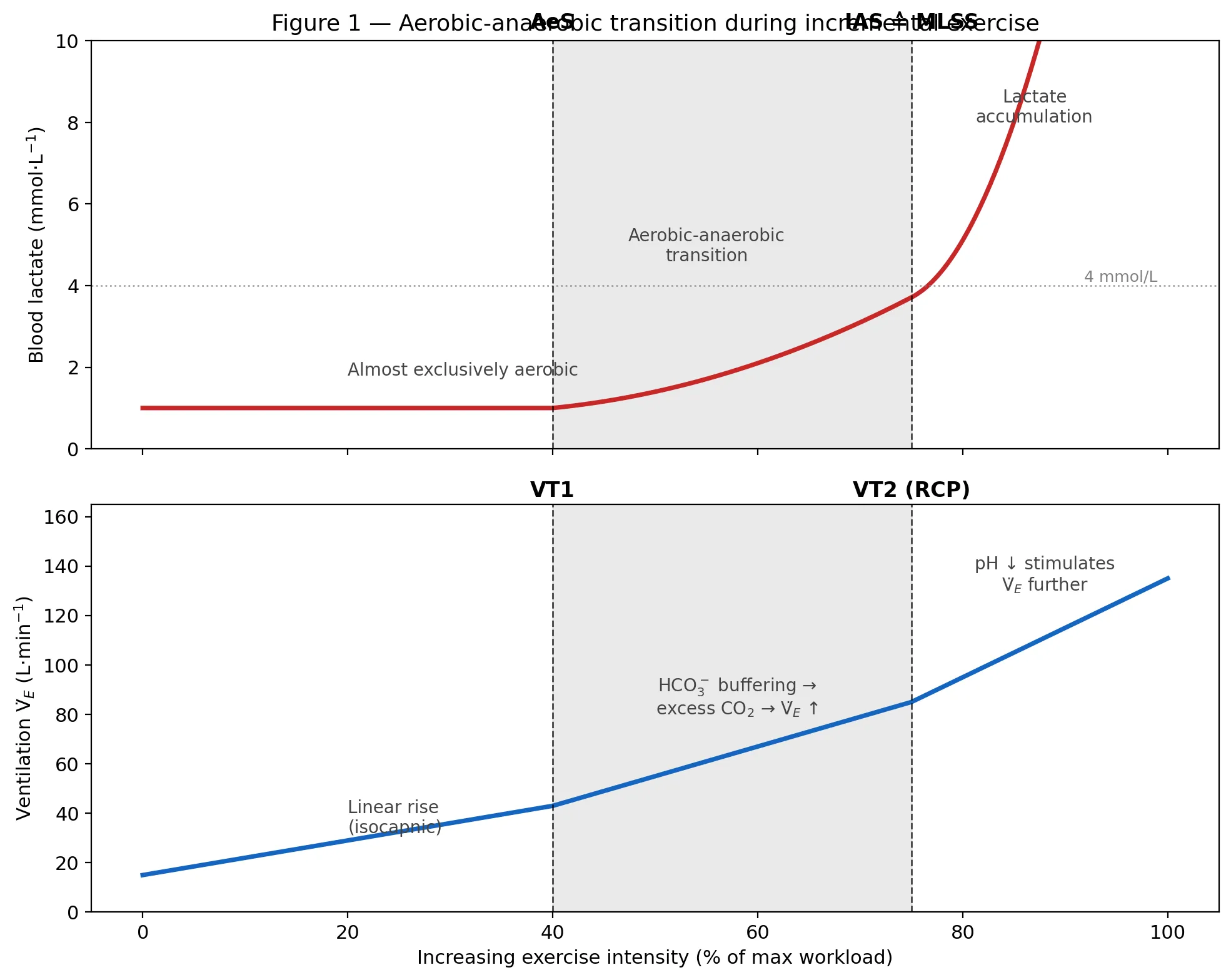
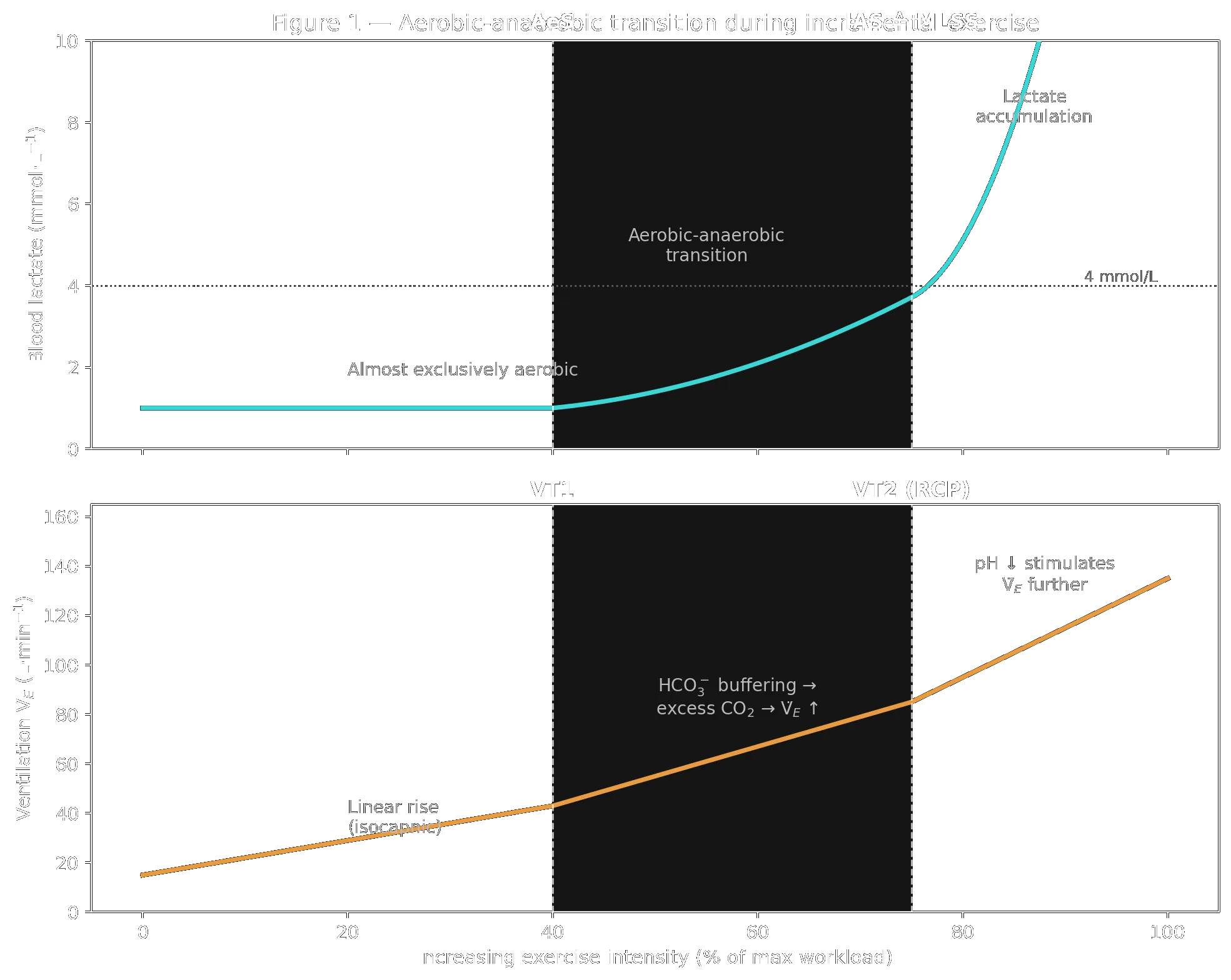
The framework introduced by Kindermann, Simon and Keul (1979) describes endurance metabolism not as one single point but as a transition zone between two breakpoints (Faude et al. 2009; Kindermann 2004):
- Aerobic threshold (AeS / LTAer): the lowest intensity at which blood lactate (bLa) first rises above baseline. Below this point the energy supply is almost exclusively oxidative; exercise can be maintained for hours.
- Anaerobic threshold (IAS / LTAn / MLSS): the upper border of the transition zone. It represents the highest workload at which lactate production and elimination are still in equilibrium — the Maximal Lactate Steady State (MLSS). Above this intensity, lactate accumulates progressively despite constant load and exhaustion follows within minutes to about an hour.
The anaerobic threshold is therefore not a sudden switch but the upper border of a gradual transition.
Schematic representation of the aerobic–anaerobic transition (grey zone). Top: blood-lactate curve with aerobic threshold (AeS) and individual anaerobic threshold (IAS ≙ MLSS). Bottom: pulmonary ventilation with the two ventilatory thresholds VT1 and VT2 (RCP). Redrawn after Kindermann (2004).
Schematic representation of the aerobic–anaerobic transition (grey zone). Top: blood-lactate curve with aerobic threshold (AeS) and individual anaerobic threshold (IAS ≙ MLSS). Bottom: pulmonary ventilation with the two ventilatory thresholds VT1 and VT2 (RCP). Redrawn after Kindermann (2004).
1.2 The MLSS as gold standard
The MLSS is determined by performing several constant-load trials of at least 30 minutes on different days at different intensities. The MLSS criterion most commonly used is: blood lactate must not rise by more than 1 mmol/L between minute 10 and minute 30 of the constant-load test (Faude et al. 2009).
At the MLSS, oxygen uptake, CO₂ output, respiratory exchange ratio and bicarbonate concentration remain approximately constant; respiratory rate and heart rate, however, drift upwards.
1.3 The 4 mmol/L threshold and its limits
Historically, Mader et al. (1976) and Heck et al. (1985) proposed a fixed threshold at 4 mmol/L lactate (LT4 / OBLA — Onset of Blood Lactate Accumulation) as a practical estimate of MLSS. Kindermann (2004) notes that the anaerobic threshold lies on average around 4 mmol/L — but in endurance-trained athletes mostly lower.
The problem with a fixed value is biological variability. Reported MLSS lactate concentrations span from about 2 to 10 mmol/L between individuals (Faude et al. 2009). Equal lactate concentrations therefore do not necessarily represent equal metabolic situations.
For this reason, individual anaerobic threshold (IAT) concepts were developed (Stegmann et al. 1981; Keul et al.; Simon et al.; Dickhuth et al.). They take the shape of the individual lactate–performance curve into account (e.g. tangent methods, +1.5 mmol/L above minimum lactate equivalent, Dmax/Dmod methods).
1.4 Agreement between LT concepts and MLSS — limits of agreement
Correlations between threshold concepts and MLSS are high, but correlations alone do not tell us whether two methods agree in absolute terms. Faude et al. (2009) recommend reporting the mean bias and the 95 % limits of agreement (LoA) according to Bland and Altman. Recalculated from raw data of Heck et al. they reported (Table VI in Faude et al. 2009):
Agreement of threshold concepts across exercise protocols (bias and 95 % limits of agreement).
| Threshold concept | Treadmill, 3-min stages | Treadmill, 5-min stages | Cycle ergometry, 2-min stages |
|---|---|---|---|
| LT4 | bias −0.13 m/s, LoA ≈ 8 % | bias +0.02 m/s, LoA ≈ 9 % | bias −19.8 W, LoA ≈ 14 % |
| IAT (Keul) | bias −0.20 m/s, LoA ≈ 9 % | bias +0.06 m/s, LoA ≈ 8 % | bias −21.0 W, LoA ≈ 11 % |
| IAT (Stegmann) | bias −0.03 m/s, LoA ≈ 12 % | bias −0.03 m/s, LoA ≈ 9 % | bias −15.0 W, LoA ≈ 18 % |
| IAT (Bunc) | bias −0.33 m/s, LoA ≈ 8 % | bias −0.14 m/s, LoA ≈ 9 % | bias −71.4 W, LoA ≈ 27 % |
Agreement of threshold concepts across exercise protocols (bias and 95 % limits of agreement).
Interpretation: even when the mean bias is small, the 95 % LoA can reach 10–20 % of the MLSS. For any individual subject the difference between a single LT estimate and the true MLSS may therefore be substantial — particularly on the cycle ergometer.
Key take-away. The anaerobic threshold is best defined functionally as the MLSS — the highest constant workload at which lactate is still in steady state. The widely used 4 mmol/L value is an average, not a biological constant. Individualised concepts narrow the bias but do not eliminate substantial 95 % LoA.
2. Worked example: determining the IAT after Stegmann et al. (1981)
2.1 Rationale of the method
The individual anaerobic threshold (IAT) after Stegmann, Kindermann and Schnabel (1981) is one of the best-validated approaches and the one most consistently shown to track the MLSS (see Section 1.4 and Faude et al. 2009). Its idea is elegant:
- The lactate curve during incremental exercise alone cannot tell us where the steady-state limit lies, because the test is too short for steady state to develop.
- The recovery lactate curve, however, contains additional information: it reflects how the organism handles the net lactate load accumulated during the last exercise stages.
- A tangent constructed from the descending recovery curve at the point where blood lactate has returned to its end-of-exercise value (L_end) to the ascending exercise curve identifies the intensity at which lactate production and elimination are still in equilibrium.
The tangent contact on the exercise curve is the IAT.
2.2 Sample protocol — incremental treadmill test
The following example uses a standard protocol that meets Stegmann’s original methodology (Faude et al. 2009).
Protocol specification for the worked lactate example.
| Parameter | Specification |
|---|---|
| Subject | Recreational male runner, 30 yr, 72 kg |
| Ergometer | Motorised treadmill, 1 % incline |
| Warm-up | 10 min jogging at ≈ 2.0 m/s |
| Stages | 6 incremental stages of 3 min each (Stegmann’s original duration) |
| Initial velocity | 2.0 m/s (7.2 km/h) |
| Increment | +0.5 m/s per stage |
| Termination | Volitional exhaustion |
| Blood sampling | 20 μL capillary blood from hyperaemised earlobe at the end of each stage and at min 1, 3, 5, 8, 10 of passive recovery |
| Analysis | Enzymatic-amperometric lactate analyser (haemolysed whole blood) |
Protocol specification for the worked lactate example.
2.3 Measured data
Incremental stage data: velocity, heart rate and lactate.
| Stage | t (min) | v (m/s) | v (km/h) | HR (bpm) | Lactate (mmol·L⁻¹) |
|---|---|---|---|---|---|
| 1 | 3 | 2.0 | 7.2 | 118 | 1.0 |
| 2 | 6 | 2.5 | 9.0 | 132 | 1.3 |
| 3 | 9 | 3.0 | 10.8 | 145 | 1.8 |
| 4 | 12 | 3.5 | 12.6 | 158 | 2.6 |
| 5 | 15 | 4.0 | 14.4 | 172 | 4.4 |
| 6 (end) | 18 | 4.5 | 16.2 | 188 | 9.0 = L_end |
Incremental stage data: velocity, heart rate and lactate.
Post-exercise lactate recovery samples.
| Recovery sample | t after exercise (min) | Lactate (mmol·L⁻¹) |
|---|---|---|
| R1 | 1 | 10.0 (= L_max) |
| R2 | 3 | 8.8 |
| R3 | 5 | 7.0 |
| R4 | 8 | 5.0 |
| R5 | 10 | 3.5 |
Post-exercise lactate recovery samples.
2.4 Construction of the IAT
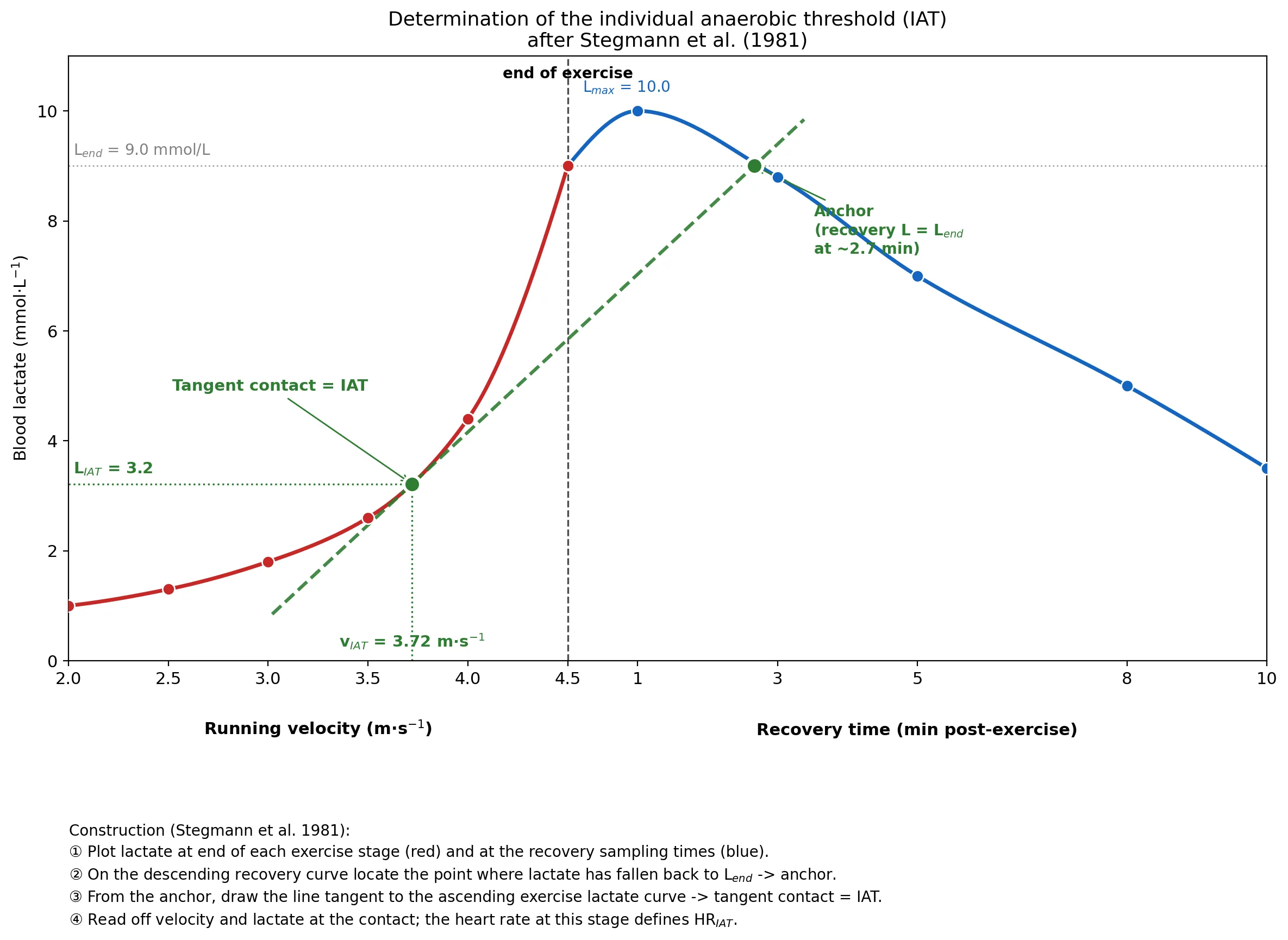
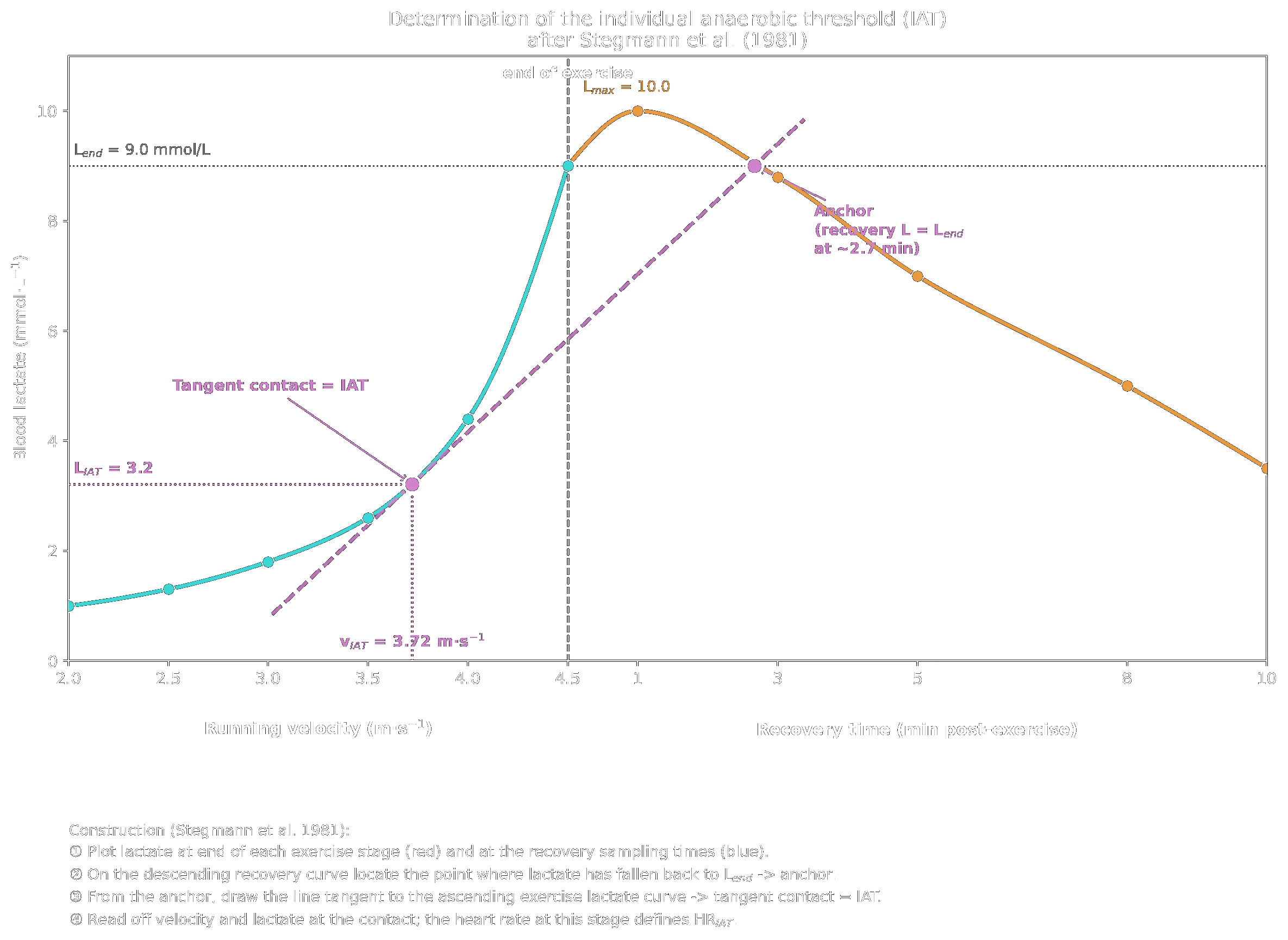
Lactate–velocity curve during incremental exercise (red) and lactate–time curve during recovery (blue). The dashed grey line marks L_end. The descending recovery curve crosses L_end at ≈ 2.7 min post-exercise (linear interpolation between R1 = 10.0 mmol/L at 1 min and R2 = 8.8 mmol/L at 3 min → L = 9.0 at t ≈ 2.7 min): this is the anchor. The dashed green line is the tangent from the anchor to the ascending exercise curve; the tangent contact on the exercise curve is the IAT. Vertical and horizontal projections give v_IAT and L_IAT respectively.
Lactate–velocity curve during incremental exercise (red) and lactate–time curve during recovery (blue). The dashed grey line marks L_end. The descending recovery curve crosses L_end at ≈ 2.7 min post-exercise (linear interpolation between R1 = 10.0 mmol/L at 1 min and R2 = 8.8 mmol/L at 3 min → L = 9.0 at t ≈ 2.7 min): this is the anchor. The dashed green line is the tangent from the anchor to the ascending exercise curve; the tangent contact on the exercise curve is the IAT. Vertical and horizontal projections give v_IAT and L_IAT respectively.
Step-by-step:
- End-of-exercise lactate. L_end = 9.0 mmol·L⁻¹ at v_end = 4.5 m/s, HR_end = 188 bpm.
- Anchor on recovery curve. Find t* where the recovery lactate has decreased back to L_end. With R1 = 10.0 mmol/L at 1 min and R2 = 8.8 mmol/L at 3 min, linear interpolation gives:
- t* = 1 + (10.0 − 9.0)/(10.0 − 8.8) × (3 − 1) = 1 + 1.7 ≈ 2.7 min post-exercise.
- Draw tangent. From the anchor at (2.7 min post, 9.0 mmol/L) draw the line tangent to the ascending exercise lactate curve.
- Read off the IAT. The tangent touches the exercise curve at approximately:
- v_IAT ≈ 3.7 m/s (13.4 km/h)
- L_IAT ≈ 3.2 mmol/L
- Interpolate the threshold heart rate. Linear interpolation between stage 4 (v = 3.5, HR = 158 bpm) and stage 5 (v = 4.0, HR = 172 bpm) at v = 3.72 m/s:
- HR_IAT ≈ 158 + (3.72 − 3.5)/(4.0 − 3.5) × (172 − 158) = 158 + 0.44 × 14 = ≈ 164 bpm.
The aerobic threshold (AeS) in the same test would be read off as the first systematic rise of lactate above baseline — in this subject between stages 3 and 4. Conventionally, this is set at v ≈ 3.0 m/s, HR ≈ 145 bpm, L ≈ 1.8 mmol/L.
2.5 Derived training prescription
Using the IAT values for this subject as the anchor (Kindermann 2004; see also Section 4 below):
Training zones derived from the individual anaerobic threshold.
| Training zone | % IAT velocity | Target velocity | Target HR | Typical lactate | Example session |
|---|---|---|---|---|---|
| Regenerative | < 70 % | < 2.6 m/s (< 9.4 km/h) | < 115 bpm | < 1.5 mmol/L | 30–45 min easy jog at 2.3 m/s (8.3 km/h) |
| Extensive endurance (GA I) | 70 – 90 % | 2.6 – 3.35 m/s (9.4 – 12.1 km/h) | 115 – 148 bpm | 1.5 – 3 mmol/L | 60–90 min steady run at 3.0 m/s (10.8 km/h), HR ~140 bpm |
| Intensive endurance (GA II / TDL) | 90 – 100 % | 3.35 – 3.72 m/s (12.1 – 13.4 km/h) | 148 – 164 bpm | 3 – 5 mmol/L | 30–45 min tempo run at 3.5 m/s (12.6 km/h), HR ~156 bpm |
| Interval training (IVT) | > 100 % | > 3.72 m/s (> 13.4 km/h) | > 164 bpm (HR drifts during the interval) | typically > 5 mmol/L | 6 × 1000 m at 4.0 m/s (14.4 km/h), 3 min jog rest |
Training zones derived from the individual anaerobic threshold.
Notes for the coach.
- Use heart rate as the primary online control parameter (it tracks workload well, is unaffected by beta-blockers, and is far more practical than repeated lactate sampling).
- For interval sessions, target HR is reached during the work bout, not from the start: prescription is normally given as work velocity ± rest interval rather than as HR.
- Re-test every 6–8 weeks of focused training. A higher v_IAT at the same HR_IAT — or the same v_IAT at a lower HR — indicates positive adaptation.
Key take-away. A single 18-minute incremental test plus 10 minutes of recovery sampling yields, via the Stegmann tangent, an individual threshold velocity, lactate concentration and heart rate. From these three numbers a complete training-zone prescription can be derived.
3. The anaerobic threshold as a metabolic, hormonal and immunological breakpoint
Although the transition between aerobic and anaerobic metabolism is gradual, clearly identifiable changes in several physiological systems coincide with the anaerobic threshold (Kindermann 2004; Faude et al. 2009):
- Metabolic. Above the IAT, lactate concentration rises continuously during constant-load exercise; bicarbonate-buffered H⁺ ions can no longer be fully compensated and pH falls, additionally stimulating ventilation. The respiratory compensation point (VT2) marks this ventilatory consequence and lies in the region of the anaerobic lactate threshold.
- Hormonal. Plasma catecholamines (adrenaline and noradrenaline) rise disproportionately when the anaerobic threshold is exceeded. Faude et al. (2009) summarise: “exercise above the MLSS is associated with an over-proportional excretion of stress hormones […] during constant-load exercise.”
- Immunological. Above the anaerobic threshold, immunological parameters such as natural killer (NK) cells and the oxidative burst of neutrophils show significant quantitative changes (Kindermann 2004).
- Neuromuscular. Lucia et al. observed changes in EMG activity of vastus lateralis and rectus femoris that coincided with the aerobic–anaerobic transition in elite male cyclists (cited in Faude et al. 2009).
These convergent breakpoints justify the concept even though “threshold” is, strictly speaking, a didactic simplification of a continuous process.
Key take-away. The anaerobic threshold marks an intensity at which not only lactate kinetics but also stress-hormone responses, immune-cell behaviour and neuromuscular activation patterns change qualitatively. It is therefore far more than a “lactate phenomenon”.
4. Exercise prescription based on the anaerobic threshold
4.1 Training zones derived from the aerobic–anaerobic transition (Kindermann 2004)
Endurance training zones and lactate guidance (German terminology).
| Zone (German terminology) | Intensity prescription | Lactate guidance |
|---|---|---|
| Regenerative training | < AeS | At/below first lactate rise |
| Extensive endurance (GA I) | ≈ 70 – < 90 % of IAT | between AeS and just below IAT |
| Intensive endurance (GA II, “Tempodauerlauf”) | 90 – 100 % of IAT | up to MLSS, typically 3–5 mmol/L in trained runners |
| Interval training (IVT) | > 100 % of IAT | suprathreshold, lactate dependent on work/rest ratio |
Endurance training zones and lactate guidance (German terminology).
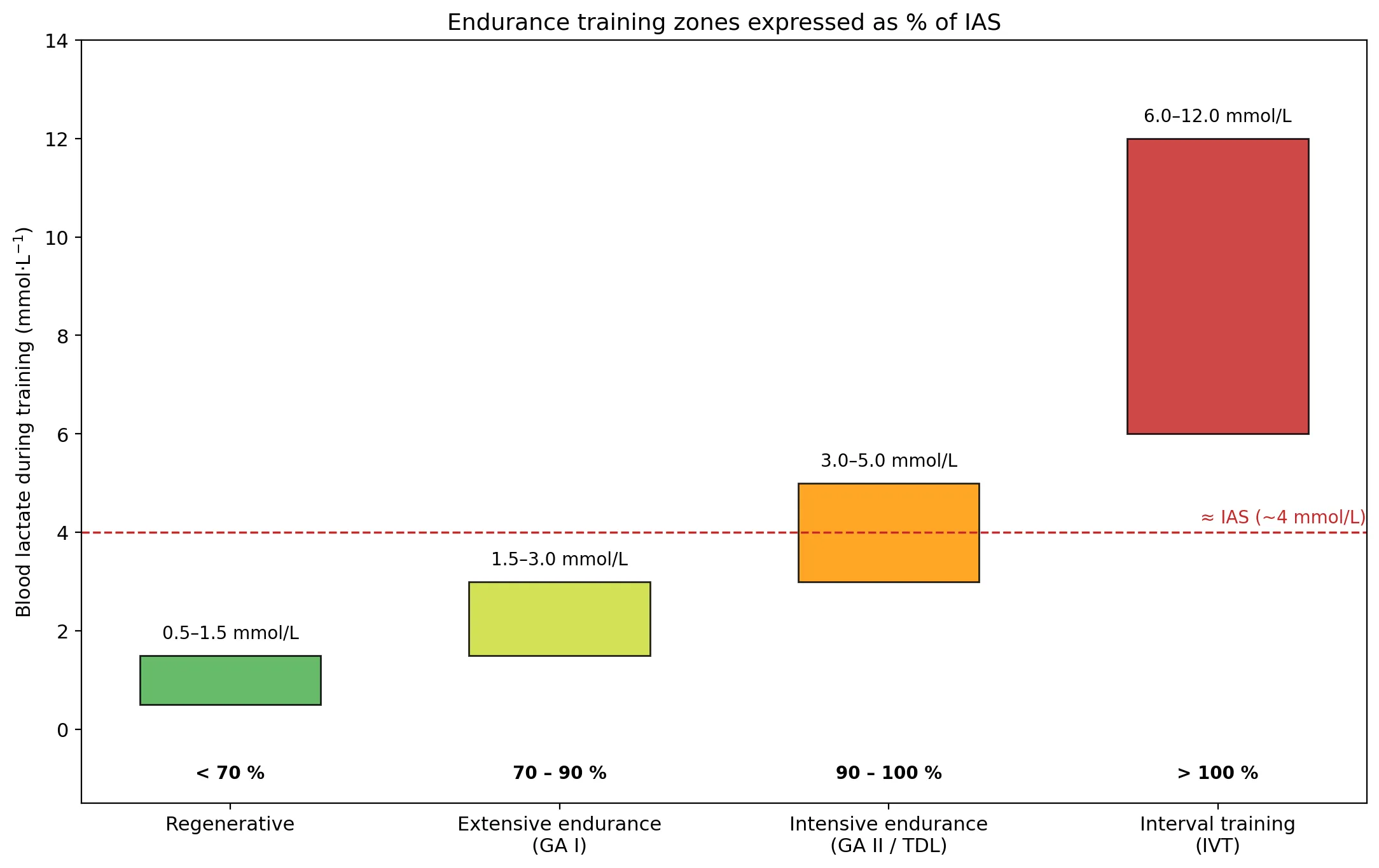
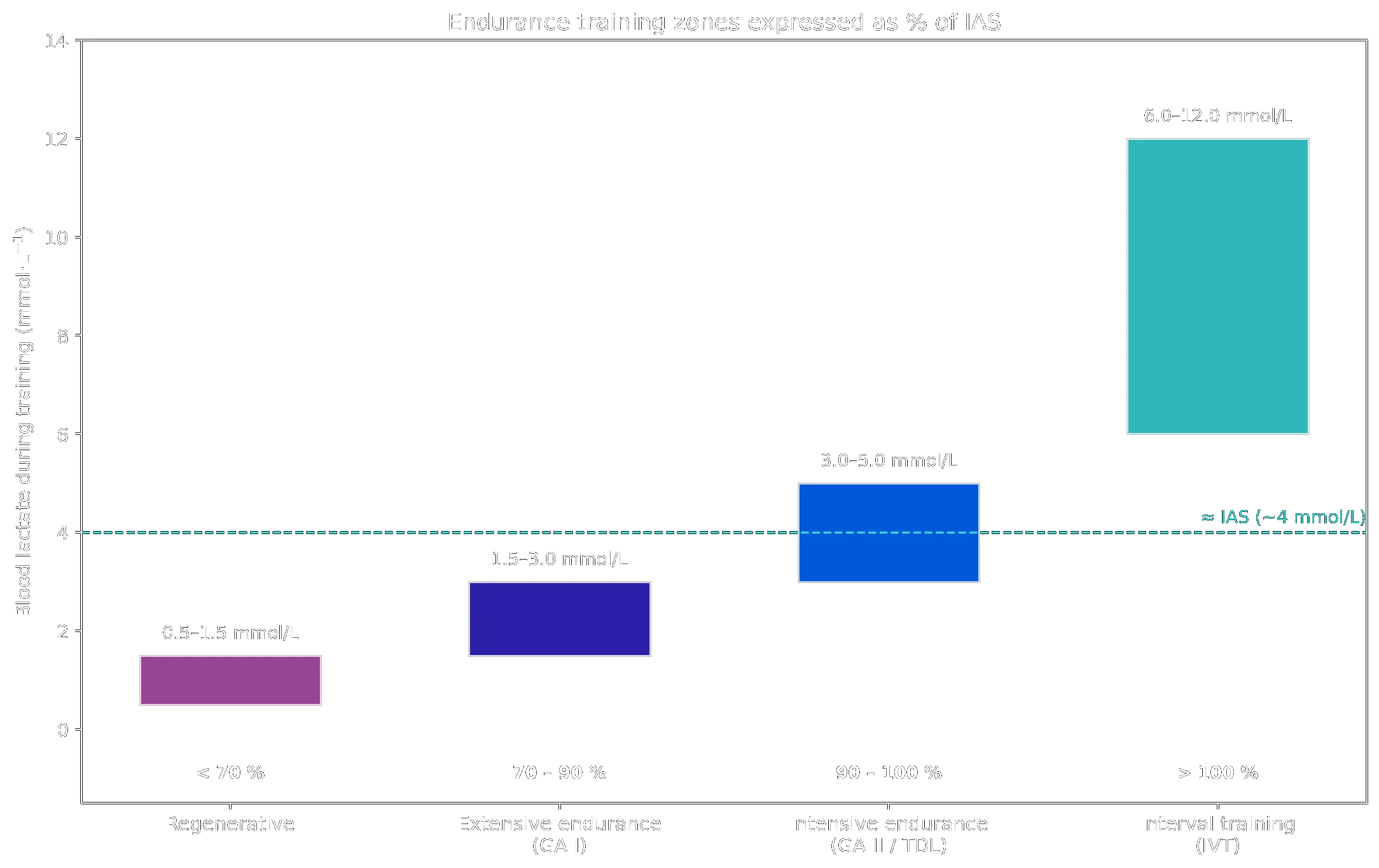
Typical blood-lactate ranges encountered during the four endurance-training zones, expressed as a percentage of the individual anaerobic threshold (IAS). Redrawn after Kindermann (2004).
Typical blood-lactate ranges encountered during the four endurance-training zones, expressed as a percentage of the individual anaerobic threshold (IAS). Redrawn after Kindermann (2004).
Heart-rate prescription is preferred in practice, because heart rate is easy to monitor and lactate response is not affected by beta-blockers — exact heart-rate targets at the IAT can therefore be given even to cardiac patients on beta-blockade.
4.2 Application examples (Kindermann 2004)
- Good marathon runners race at the IAT. Marathon time can be predicted from running speed at the threshold. Regional-class runners (~3 h) run at ~95 % of IAT speed; elite runners ~100 %.
- Fat oxidation is maximal in absolute terms at 55–72 % VO₂max, corresponding to 68–79 % HRmax — i.e. within the aerobic–anaerobic transition. Training around ~90 % of the IAT therefore also elicits maximal fat oxidation.
- Preventive / rehabilitative sport. Short sessions can be performed between 90 and 100 % of the IAT, longer sessions close to the AeS. Suprathreshold work is not relevant for health sport and may be risky for patients.
4.3 The ACSM/ESSA framework (Bishop et al. 2025)
The recent joint ACSM/ESSA expert statement proposes five intensity categories anchored on metabolic thresholds — the first metabolic threshold (MT1) being approximated by the first lactate threshold/AeS, and the second metabolic threshold (MT2) being approximated by the MLSS or critical power/speed:
Cardiorespiratory intensity categories by physiological marker.
| Category | Cardiorespiratory exercise reference |
|---|---|
| Very low | no current physiological marker |
| Low | below MT1 |
| Moderate | above MT1 but below MT2 |
| High | above MT2 but below Wmax (work rate at VO₂max) |
| Very high | above Wmax |
Cardiorespiratory intensity categories by physiological marker.
Bishop et al. (2025) state that the direct measurement of metabolic thresholds plus Wmax is “the best and preferred method to define exercise-intensity categories that will produce similar physiological stresses in individuals with different exercise capacities.”
Key take-away. The anaerobic threshold subdivides the endurance-training continuum into physiologically distinct zones. Heart-rate-controlled prescription anchored on the IAT (or on MT1/MT2) yields more comparable metabolic stress between individuals than work-rate or %VO₂max prescription.
5. Trained versus untrained subjects
The anaerobic threshold is more sensitive to training than VO₂max (Kindermann 2004; Faude et al. 2009):
- Absolute power/velocity at MLSS is markedly higher in trained subjects — the entire lactate–performance curve shifts to the right.
- Relative to VO₂max, the IAT lies between roughly 60 and 85 % VO₂max, depending on sport and training state (AeS roughly 40–65 % VO₂max). Highly trained endurance athletes operate at the upper end of this range.
- Lactate concentration at the MLSS is lower in endurance-trained athletes than in untrained subjects. Faude et al. (2009) explicitly warn that the LT4 (4 mmol/L) “may frequently underestimate (particularly in anaerobically trained subjects) or overestimate (in aerobically trained athletes) real endurance capacity.”
- VO₂max alone fails to discriminate between subjects of homogeneous performance level (e.g. between elite endurance runners). The threshold, however, retains discriminatory power and correlates strongly with competition performance.
- Training adaptations (mitochondrial density, oxidative enzymes, capillarisation, fibre-type shifts) shift the curve to the right — this is detected sensitively by changes at the IAT, often before VO₂max changes.
Key take-away. Training shifts the IAT to higher absolute workloads and tends to lower the lactate concentration at which the MLSS occurs. The IAT is a more sensitive marker of endurance training adaptations than VO₂max — especially in already-trained populations.
6. The anaerobic threshold and percentages of VO₂max / HRmax
6.1 Typical values
Across studies summarised by Kindermann (2004):
- AeS: ~40 – 65 % VO₂max
- IAT: ~60 – 85 % VO₂max
- Maximum fat oxidation: 55 – 72 % VO₂max ≈ 68 – 79 % HRmax (within the aerobic–anaerobic transition)
6.2 Why %VO₂max / %HRmax are not a reliable prescription tool
Although these percentages are convenient, all three reviewed papers stress that a fixed percentage of VO₂max or HRmax does not produce the same metabolic strain in different people:
- Meyer, Gabriel and Kindermann (1999, cited in Kindermann 2004) showed that exercise intensity prescriptions based on %VO₂max or %HRmax are inadequate because the IAT corresponds to a wide range of these percentages.
- Bishop et al. (2025) cite a study reporting a 40-fold range in the increase of muscle lactate between subjects at 70 % of VO₂max. At 80 % of HRmax, approximately half the participants were above their first metabolic threshold and approximately half were below.
- Faude et al. (2009) likewise note that LTs are superior to VO₂max for assessing endurance performance in homogeneous groups of athletes.
- Bishop et al. (2025) conclude that “prescribing exercise intensity based on a fixed percentage of maximal anchors (e.g., %VO₂max, %VO₂R, %HRmax, or %HRR) will cause individuals to exercise in different training intensity categories and to experience large variations in metabolic stress.”
Key take-away. %VO₂max and %HRmax are practical descriptors of where the threshold tends to lie in a population, but they are not adequate prescription anchors for individuals. Threshold-based prescription (heart rate at the IAT, or thresholds derived from a GXT) achieves more comparable physiological strain.
7. Strengths and weaknesses of the anaerobic-threshold concept
7.1 Strengths
- High correlation with endurance performance. Of 32 studies reviewed by Faude et al. (2009), the overwhelming majority reported strong linear correlations of LTs with running competition performance, with r-values typically between 0.7 and 0.98 and common variance of 55 – 85 %.
- Sensitivity to training. Threshold-based parameters change earlier and more clearly than VO₂max, especially in trained athletes (Kindermann 2004).
- Independence of motivation / exhaustion. Unlike VO₂max, the IAT does not require an all-out effort and can therefore be used safely in patients and recreational subjects (Kindermann 2004; Bishop et al. 2025).
- Reproducibility. Test–retest reliability for velocity or power at LTs is high (r > 0.9 across LTfix, LTAer and LTAn concepts); VO₂ at LT is slightly lower (r ≈ 0.8 – 0.9) (Faude et al. 2009).
- Practical, multi-system breakpoint. Metabolic, hormonal, immunological and neuromuscular changes converge at this intensity, giving the concept biological plausibility.
- Robust against beta-blockade. Lactate–performance curves are not influenced by beta-blockers, so threshold-based heart-rate prescriptions remain valid in cardiac patients (Kindermann 2004).
7.2 Weaknesses
- Definitional confusion. Faude et al. (2009) located 25 different LT concepts in the literature. Threshold values obtained by different methods are generally not comparable. Many concepts are insufficiently validated.
- The term “threshold” is misleading. Aerobic and anaerobic pathways always contribute simultaneously; the transition is continuous, not abrupt. The model is appropriate didactically and practically but should not be reified.
- Methodological dependence. Threshold values depend on:
- test protocol (stage duration, work-rate increment, ramp vs step);
- blood-sampling site (earlobe vs fingertip);
- blood medium analysed (plasma vs whole blood vs capillary);
- lactate analyser type and ambient conditions;
- nutritional state — glycogen depletion shifts the lactate curve down and can be misread as an improvement (Faude et al. 2009).
- Substantial individual differences from MLSS. Even for the best-validated concepts, 95 % LoA between an LT estimate and the MLSS reach ~10 % on a treadmill and up to ~27 % on a cycle ergometer for some methods (Faude et al. 2009).
- MLSS lactate concentration varies between 2 and 10 mmol/L across individuals — fixed values such as 4 mmol/L are at best a population average.
- MLSS reproducibility itself is not well established. Faude et al. (2009) explicitly note “no scientific data” on the basic variability of MLSS, which limits how strictly LTs can be judged.
- Limited evidence outside running. Validation against competition performance is strong for running but more heterogeneous in cycling and sparse in other endurance sports.
- Limited applicability to large populations. Bishop et al. (2025) note that threshold-based testing requires expensive equipment, time-consuming protocols, blood sampling and expert interpretation — not realistic for population-level prescription.
Key take-away. The anaerobic-threshold concept is a powerful, valid and reliable instrument when (1) the chosen LT concept matches the question, (2) the test protocol is standardised, and (3) results are interpreted on the level of individuals with appropriate confidence intervals — not as point estimates carved in stone.
8. Summary in one paragraph
The anaerobic threshold is the upper border of the aerobic–anaerobic transition and, functionally, corresponds to the maximal lactate steady state. Although it averages around 4 mmol/L of blood lactate, the actual MLSS concentration varies between 2 and 10 mmol/L between individuals, making individualised threshold concepts preferable to fixed values; even so, 95 % limits of agreement with the gold-standard MLSS reach 10–20 %. The threshold is more than a metabolic marker: catecholamines, NK-cell activity and oxidative burst all change disproportionately above this intensity, so it is best regarded as a multi-system breakpoint. It is the central anchor for endurance-training prescription, with regenerative, extensive (GA I, ~70–90 % IAT), intensive (GA II / TDL, ~90–100 % IAT) and interval (>100 % IAT) zones derived from it. Trained subjects reach the threshold at higher absolute workloads and often at lower lactate concentrations than untrained subjects, and the threshold is a more sensitive marker of training adaptation than VO₂max. Although it tends to fall between 60 and 85 % VO₂max (or 68–79 % HRmax for maximal fat oxidation), fixed percentages of these maximal anchors should not be used to prescribe individual training, because identical %VO₂max or %HRmax produce widely different metabolic strains. The main strengths of the concept are reliability, independence from maximal effort, and strong correlation with endurance performance; the main weaknesses are the proliferation of incompatible definitions, methodological sensitivity, and the fact that the underlying transition is, strictly speaking, continuous.
References
-
Kindermann W. Anaerobe Schwelle. Deutsche Zeitschrift für Sportmedizin 55 (6), 2004: 161–162.
-
Faude O, Kindermann W, Meyer T. Lactate Threshold Concepts — How Valid Are They? Sports Medicine 39 (6), 2009: 469–490.
-
Bishop DJ et al. Physical Activity and Exercise Intensity Terminology — ACSM/ESSA Joint Expert Statement. Journal of Science and Medicine in Sport 28, 2025: 980–991.
One-Minute-Paper Topics
A One-Minute-Paper (OMP) is a short, focused prompt that students answer in ~60 seconds at the end of a session to consolidate learning, surface misconceptions, and provide formative feedback. When answering, be concise, specific, and use terminology from today’s session.
- Define the anaerobic threshold in terms of the maximal lactate steady state (MLSS) and explain why it represents the upper border of the aerobic–anaerobic transition rather than a single switching point.
- What MLSS criterion (in mmol/L over which time window) is most commonly used to identify the highest workload at which lactate production and elimination are still in equilibrium?
- Why is the fixed 4 mmol/L threshold (LT4 / OBLA) considered only a population average rather than a biological constant? Cite the reported between-subject range of MLSS lactate concentrations.
- Explain the rationale of the Stegmann tangent method: why does the recovery-lactate curve provide information that the incremental exercise curve alone cannot?
- In the Stegmann construction, what does the anchor point on the recovery curve represent, and how is it located on the time axis?
- Given an end-of-exercise lactate of 9.2 mmol/L with recovery values of 10.2 mmol/L at 1 min and 8.6 mmol/L at 3 min, calculate by linear interpolation the time at which the recovery curve crosses L_end.
- Why does Faude et al. (2009) recommend reporting Bland–Altman 95 % limits of agreement (LoA) rather than only Pearson correlations when comparing LT concepts against the MLSS?
- List the four endurance-training zones derived from the IAT and give their approximate percentage range of IAT velocity.
- Why is heart rate preferred over repeated blood-lactate sampling as the online control parameter for endurance training prescription in the field?
- Name three physiological systems other than lactate kinetics that show qualitative breakpoints at the anaerobic threshold.
- Explain in one sentence each how the MLSS lactate concentration and the absolute MLSS workload typically differ between endurance-trained and untrained subjects.
- Why is the IAT a more sensitive marker of endurance-training adaptation than VO₂max — especially in already-trained populations?
- Why does prescribing exercise at a fixed %VO₂max or %HRmax produce unequal metabolic stress between individuals? Cite one quantitative example from Bishop et al. (2025).
- Distinguish MT1 and MT2 in the ACSM/ESSA framework and name the physiological markers each approximates.
- List three methodological factors (test protocol, blood sampling, analysis, nutritional state) that systematically influence the position of a lactate threshold on the lactate–performance curve.
- Why can glycogen depletion lead to a misleadingly “improved” lactate–performance curve in a follow-up test, and how should this be controlled in re-testing?
- A recreational runner has v_IAT = 3.8 m/s, HR_IAT = 166 bpm, L_IAT = 4.0 mmol/L. Prescribe a 60-minute extensive endurance (GA I) session with appropriate velocity, target HR, and expected lactate range.
- Faude et al. (2009) located 25 different LT concepts in the literature. What practical problem does this proliferation create for coaches and clinicians comparing test results across labs?
- Why are threshold-based heart-rate prescriptions still valid in cardiac patients on beta-blockers, while %HRmax prescriptions are not?
- Maximal fat oxidation occurs at approximately 55–72 % VO₂max, which corresponds to roughly 90 % of the IAT. Use this to justify the training-zone choice for a client whose primary goal is weight management, and explain why prescription at the IAT itself or above would be counter-productive for this goal.