Exercise and Immune System, Limits of Performance, Energy balance
Table of Contents
- Protection Against Violation of Integrity — Immunity and Inflammatory Regulation
- What Are the Limits of Physical Performance?
- Energy Balance
- References
- One-Minute-Paper Topics
1 Protection Against Violation of Integrity — Immunity and Inflammatory Regulation
Overview of the Immune System
The immune system is the body’s primary defense against pathogens (bacteria, viruses, fungi) and endogenous threats (abnormal cells, debris). It operates through two integrated mechanisms:
Innate Immunity
- First line of defense — non-specific, immediate response.
- Components: Skin, mucous membranes, phagocytes (neutrophils, macrophages), natural killer cells, complement system.
- Responds to: Pathogen-associated molecular patterns (PAMPs).
- Characteristics: Does not require prior sensitization; activation is rapid.
Adaptive (Acquired) Immunity
- Second line of defense — specific, delayed response.
- Components: T lymphocytes (cellular immunity), B lymphocytes (humoral immunity), antibodies.
- Responds to: Specific antigens.
- Characteristics: Requires sensitization; activation is slower but generates immune memory.
Inflammation as an Immune Response
Inflammation is a protective response to tissue injury, infection, or immune challenge. It involves:
-
Immediate phase (0–15 minutes):
- Mast cells and resident macrophages release histamine and cytokines.
- Increased vascular permeability — plasma and immune cells enter tissues.
-
Early phase (15 minutes to 2 hours):
- Neutrophil recruitment (primary cell type in acute inflammation).
- Complement activation — enhances phagocytosis and inflammation.
-
Late phase (2–24 hours):
- Macrophage infiltration — phagocytosis and cleanup.
- Lymphocyte recruitment — adaptive immune response initiation.
-
Resolution phase:
- Anti-inflammatory cytokines (IL-10, TGF-β) suppress inflammation.
- Tissue repair and restoration of homeostasis.
Acute Inflammation vs. Chronic Inflammation
Acute inflammation is a protective, self-limiting response lasting hours to days. It is essential for fighting infection and initiating tissue repair.
Chronic inflammation persists for weeks to months or longer. It is detrimental to health and is implicated in:
- Cardiovascular disease
- Type 2 diabetes
- Autoimmune diseases
- Neurodegenerative diseases
- Cancer
Inflammatory Markers and Exercise
Key inflammatory markers measured in exercise physiology:
- IL-6 (Interleukin-6): Dual role — pro-inflammatory at rest; anti-inflammatory when produced by muscle during exercise (myokine).
- TNF-α (Tumor Necrosis Factor-α): Primarily pro-inflammatory; elevated in chronic disease states.
- CRP (C-Reactive Protein): Acute phase reactant; elevated with infection and chronic disease.
- IL-10: Anti-inflammatory; suppresses pro-inflammatory cytokine production.
- Cortisol: Stress hormone with immunosuppressive effects at elevated baseline levels.
Exercise Effects on Immunity and Inflammation
Acute exercise effects:
- Immune cell mobilization: Transient increase in circulating lymphocytes, neutrophils, and natural killer cells.
- IL-6 release from muscle (myokine effect): Acts as anti-inflammatory signal despite initial elevation.
- Immune surveillance enhancement: Mobilized lymphocytes migrate to tissues, enhancing pathogen detection.
Chronic exercise effects:
- Reduced resting inflammatory markers (IL-6, TNF-α, CRP).
- Enhanced immune surveillance and function — increased T-cell numbers and improved function.
- Improved antibody response to vaccination.
- Reduced infection risk in physically active individuals (U-shaped relationship with extreme endurance exercise).
Practical insight: Regular moderate-to-vigorous physical activity enhances immune competence and reduces chronic inflammation, protecting against age-related immune decline and lifestyle diseases.
2 What Are the Limits of Physical Performance?
2.1 What Influence Does the Ageing Process Have on Exercise?
Physical performance is part of the biological, psychological and social development of humans — subject to a biologically and genetically predetermined change and, on the other hand, to a change influenced to a limited extent by behaviour and circumstances, from the beginning of life to the end of it [1].
Physical performance is an important prerequisite for an active individual lifestyle. Without any noticeable restrictions, performance is accessed almost unnoticed and “as if it were a matter of course”. It is not uncommon for this “obviousness to physical performance” to be equated with vitality, well-being and health [1].
2.2 What Role Does Performance Play in Shaping One’s Life?
Physical performance is part of the biological, psychological and social development of humans throughout the lifespan. Performance capability impacts quality of life, independence, and health status. The decline in physical performance with aging is a significant public health concern, associated with increased disability, reduced autonomy, and higher mortality risk.
2.3 Physiological Definition of Physical Performance
The description of physical performance requires reference points or areas for quantitative classification. Reference ranges are based on empirical studies and on the known physiological minima and maxima. The terms “increase” and “restriction” used in this context are conventions and ostensibly descriptive in nature [1].
2.4 Sports Medical Definition of Physical Performance
From a biological-physical perspective, physical performance is the muscular body work performed in a unit of time — the sum of all determinants currently available for the provision of physical performance [1].
From the perspective of biochemical energy supply, physical performance is the aerobic and/or anaerobic energy provided by high-energy phosphates in a unit of time in order to perform neuromuscular body work [1].
2.5 Determinants of Physical Performance
From a physiological point of view, the primary determinants of performance are:
- The biological (anatomical) structure
- The physiological functionality of the biological structure
Both primary determinants relate to the level of the entire organism and sub-levels of structures, systems and control circuits. The two primary determinants are essentially influenced by secondary determinants [1]:
- (Biological) ageing processes
- Health as physiological functionality
- Disease and illness as physiological mal-/dysfunctionality
- Health- and functionality-related lifestyles
- (Lack of) nutrient supply
- Movements
- Physical activity (exercise and training in leisure, occupation and sports)
- Genetics (genotype, epigenetics)
- Environmental factors (physical, chemical, ecological, socio-economic)
- Sensomotorics and perception and psyche
When dealing with the limits of physical performance, a key question is whether the limits are of a physiological nature or caused by pathologies.
2.6 Extended Definition of Physical Performance
Beyond the narrow biological-physical definition, physical performance corresponds to the value created through physical work and energy consumption (movements, exercise, training, sport) and measured against the goal of action with a measurable result and a minimum level. Performance depends on biological, psychological and social resources, external stress and internal stress as well as the willingness to perform [1].
Limits of performance with age: relating MET, V̇O₂max, physical activity behaviour and mortality/morbidity [%] across the lifespan — from physical inactivity (1 MET, 3.5 mL·min⁻¹·kg⁻¹) to very fast running (~26 METs, ~90 mL·min⁻¹·kg⁻¹) — demonstrates age-dependent changes in maximal performance capacity.
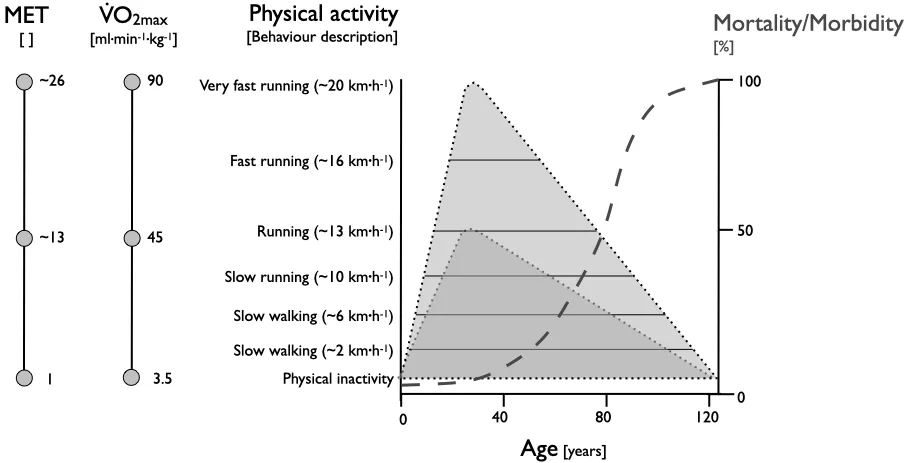
Limits of performance with age: relating MET, V̇O₂max, physical activity behaviour and mortality/morbidity [%] across the lifespan — from physical inactivity (1 MET, 3.5 mL·min⁻¹·kg⁻¹) to very fast running (~26 METs, ~90 mL·min⁻¹·kg⁻¹) — demonstrates age-dependent changes in maximal performance capacity.
2.7 How Fast Can People Run for How Long?
From a physiological point of view, a high running speed means that muscles have to provide fast and a lot of energy for muscle contractions. A low running speed requires slower contractions and a lower amount of energy per unit time.
The organism has an answer ready for high and low running speeds through different energy supply systems. However, physiological mechanisms also have their limits: after a certain period of time, muscle contraction and energy metabolism become fatigued. The faster you run, the sooner you get tired.
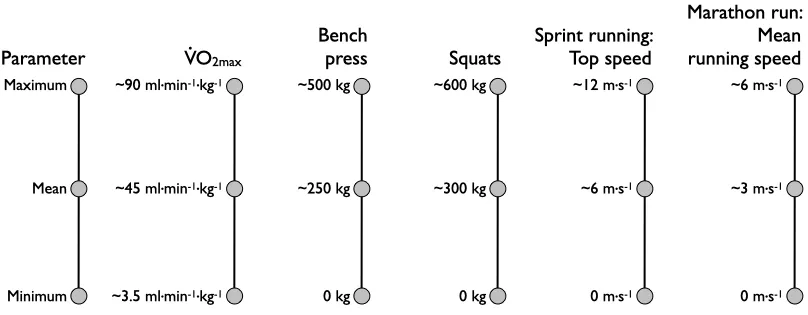
Reference performance parameters (approximate maxima):
Approximate maximal, mean and minimal reference values for selected strength and endurance performance parameters.
| Parameter | Maximum | Mean | Minimum |
|---|---|---|---|
| V̇O₂max (mL·min⁻¹·kg⁻¹) | ~90 | ~45 | ~3.5 |
| Bench press | ~500 kg | ~250 kg | 0 kg |
| Squats | ~600 kg | ~300 kg | 0 kg |
| Sprint top speed | ~12 m·s⁻¹ | ~6 m·s⁻¹ | 0 m·s⁻¹ |
| Marathon mean speed | ~6 m·s⁻¹ | ~3 m·s⁻¹ | 0 m·s⁻¹ |
Approximate maximal, mean and minimal reference values for selected strength and endurance performance parameters.
2.8 How Fast Is the Energy Supply at Different Exercise Intensities?
The speed of muscular contraction depends on the speed of energy supply [2]:
Predominant energy-supply systems as a function of effort duration, with representative sporting examples.
| Duration | Energy source(s) | Examples |
|---|---|---|
| Few seconds (<2 s) | Available ATP | Power lift, high jump, javelin throw, golf swing, tennis serve |
| Up to 6–8 seconds | ATP + creatine phosphate (PCr) | Sprints, fast breaks, gymnastics routine |
| Up to ~90 seconds | ATP + PCr + anaerobic glycolysis (lactate formation) | Long sprints 200–400 m, 100 m swimming |
| ~800 m | ~50 % anaerobic + ~50 % aerobic | Middle-distance running |
| Longer distances | Aerobic glycolysis → β-oxidation (increasing proportion) | Long-distance running, endurance events |
Predominant energy-supply systems as a function of effort duration, with representative sporting examples.
Energy flow rates:
- ATP and creatine phosphate capacity: ~5 mmol·g⁻¹ | <2–3 s; ~19 mmol·g⁻¹ | <5–8 s
- Anaerobic glycolysis capacity: ~50 mmol·g⁻¹ | <60 s
- Aerobic glycolysis and β-oxidation: limited by substrates | hours to days
Energy flow rate comparison (mmol·kg⁻¹·s⁻¹):
- ATP and CP: ~3–6
- Anaerobic glycolytic: ~1.5–3
- Aerobic glycolytic: ~0.5–0.75
- Aerobic β-oxidation: ~0.24–0.4
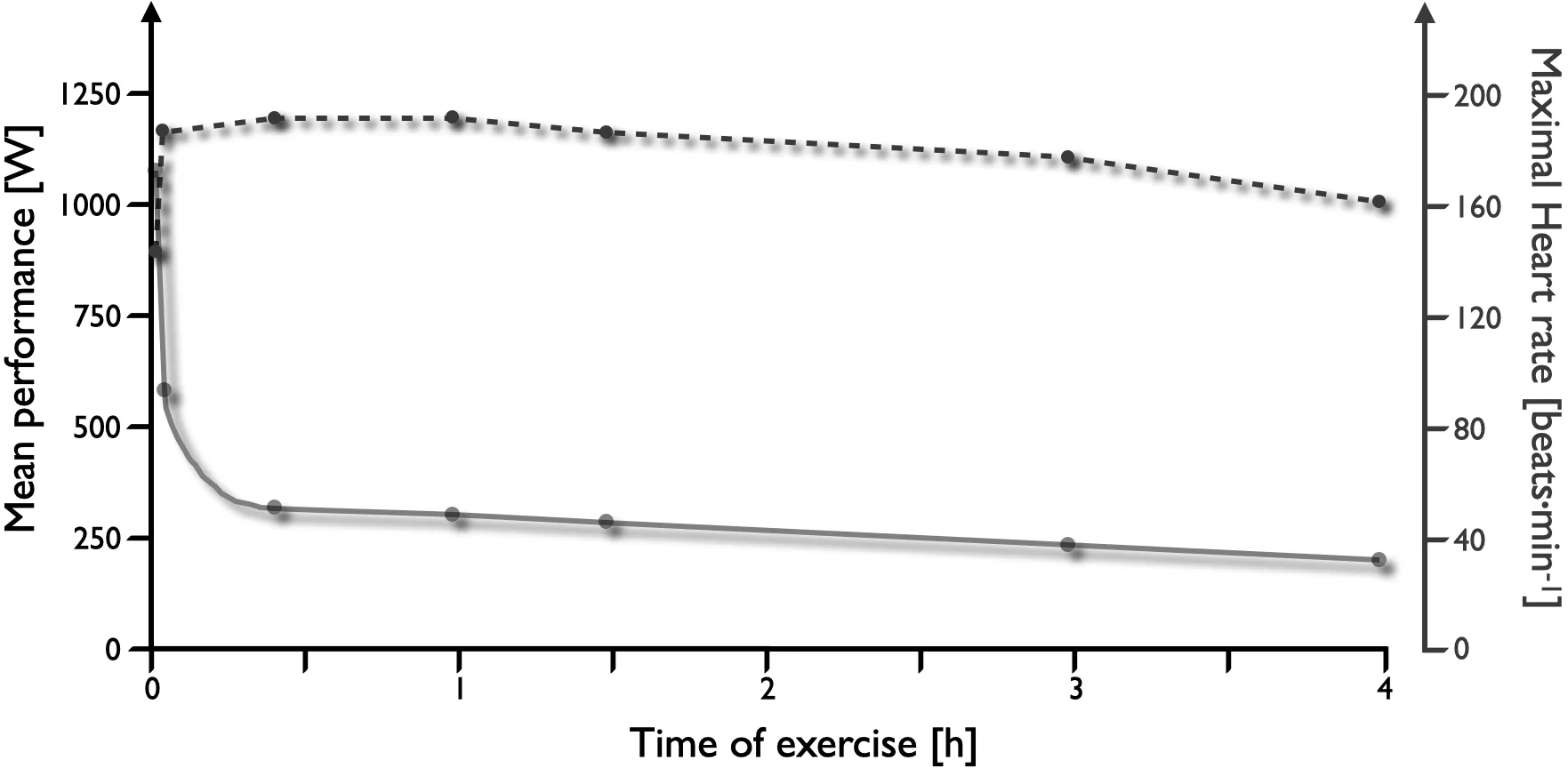
Adenosine-triphosphate (ATP) flow rates versus time. P — cycling performance on a bicycle ergometer; RPE — ratings of perceived exertion (Borg scale 6–20).
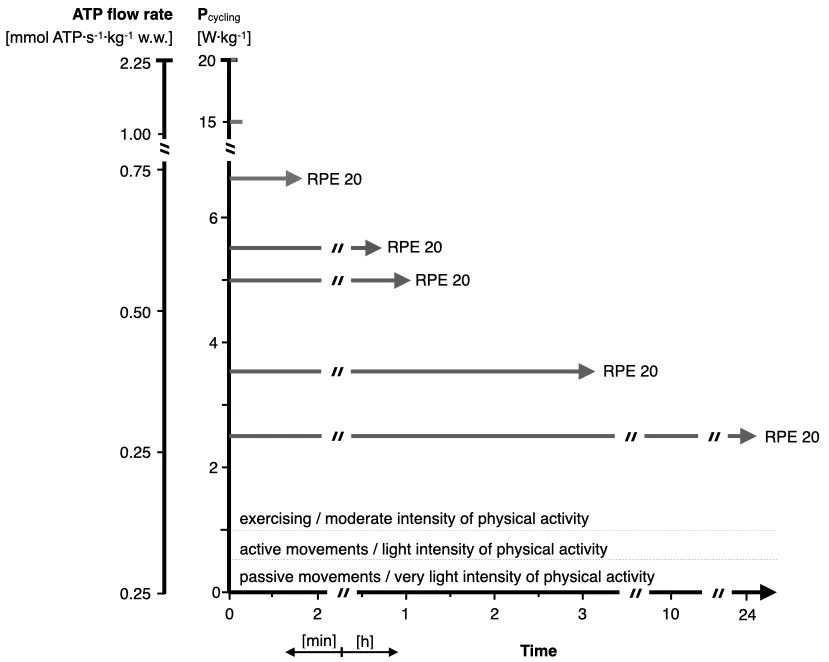
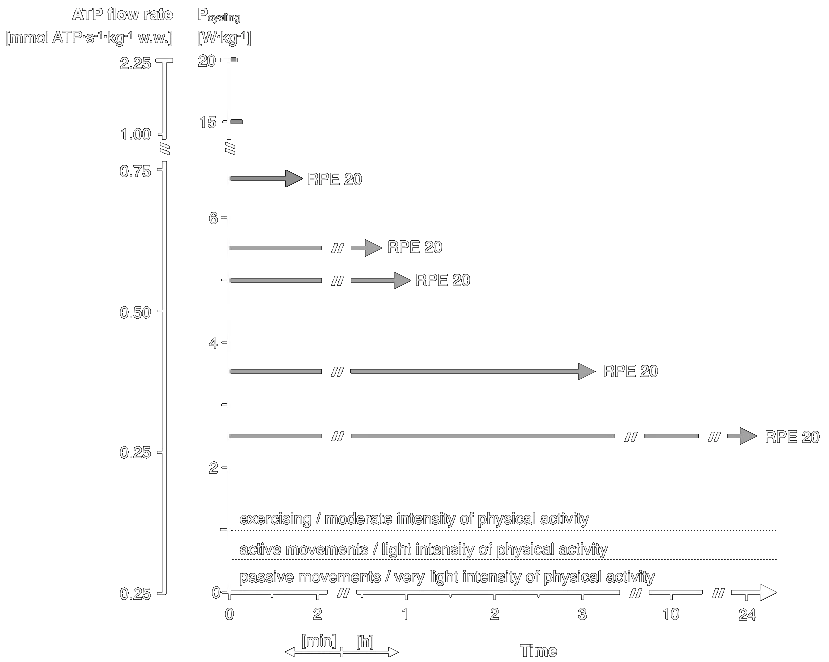
Adenosine-triphosphate (ATP) flow rates versus time. P — cycling performance on a bicycle ergometer; RPE — ratings of perceived exertion (Borg scale 6–20).
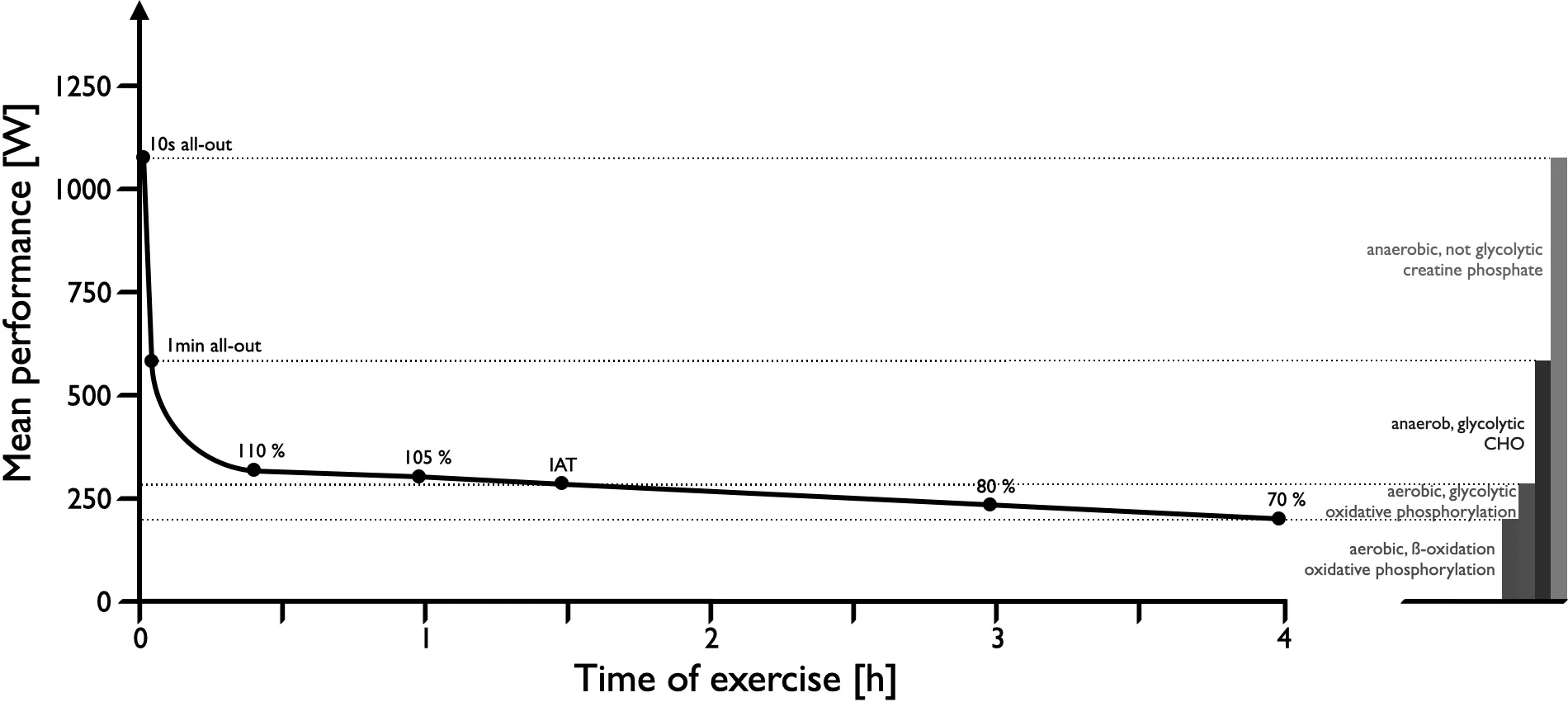
Time course of energy generation.
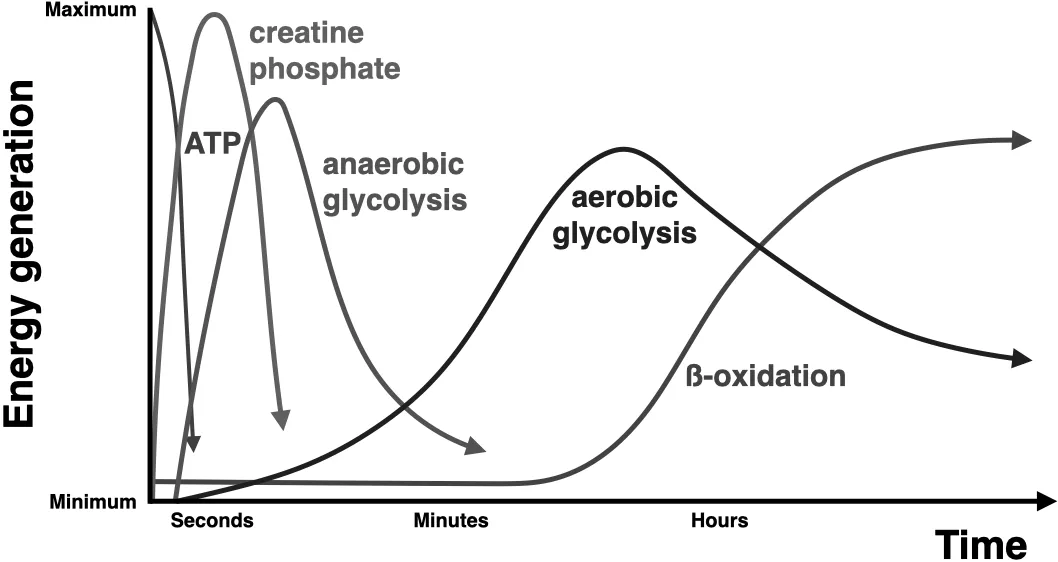
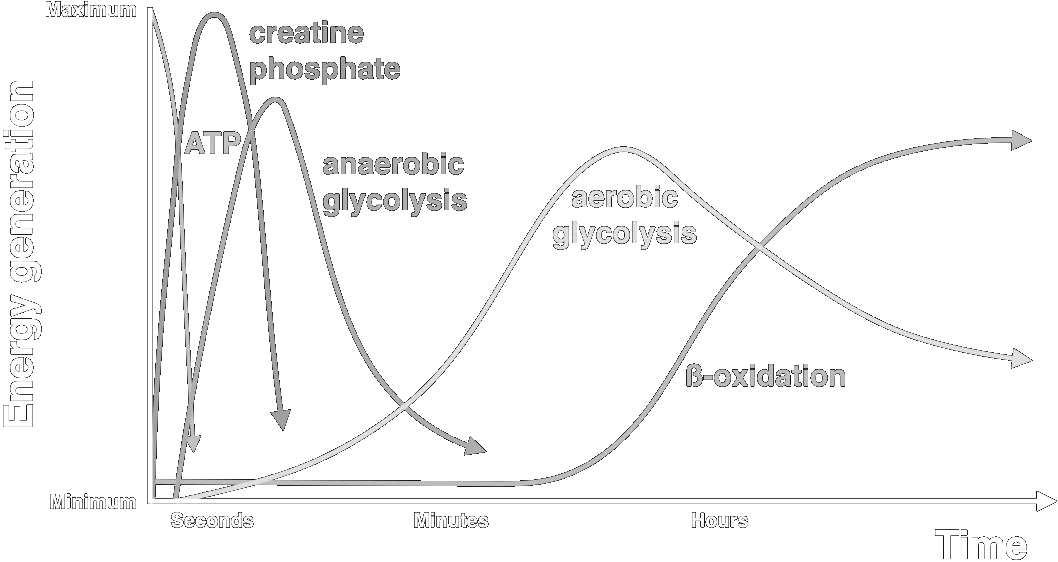
Time course of energy generation.
Cycle-ergometer exercise of different intensities and durations, showing performance, lactate generation and hormone secretion built up step by step. Male subjects with a V̇O₂max of 60–65 ml·min⁻¹·kg⁻¹.
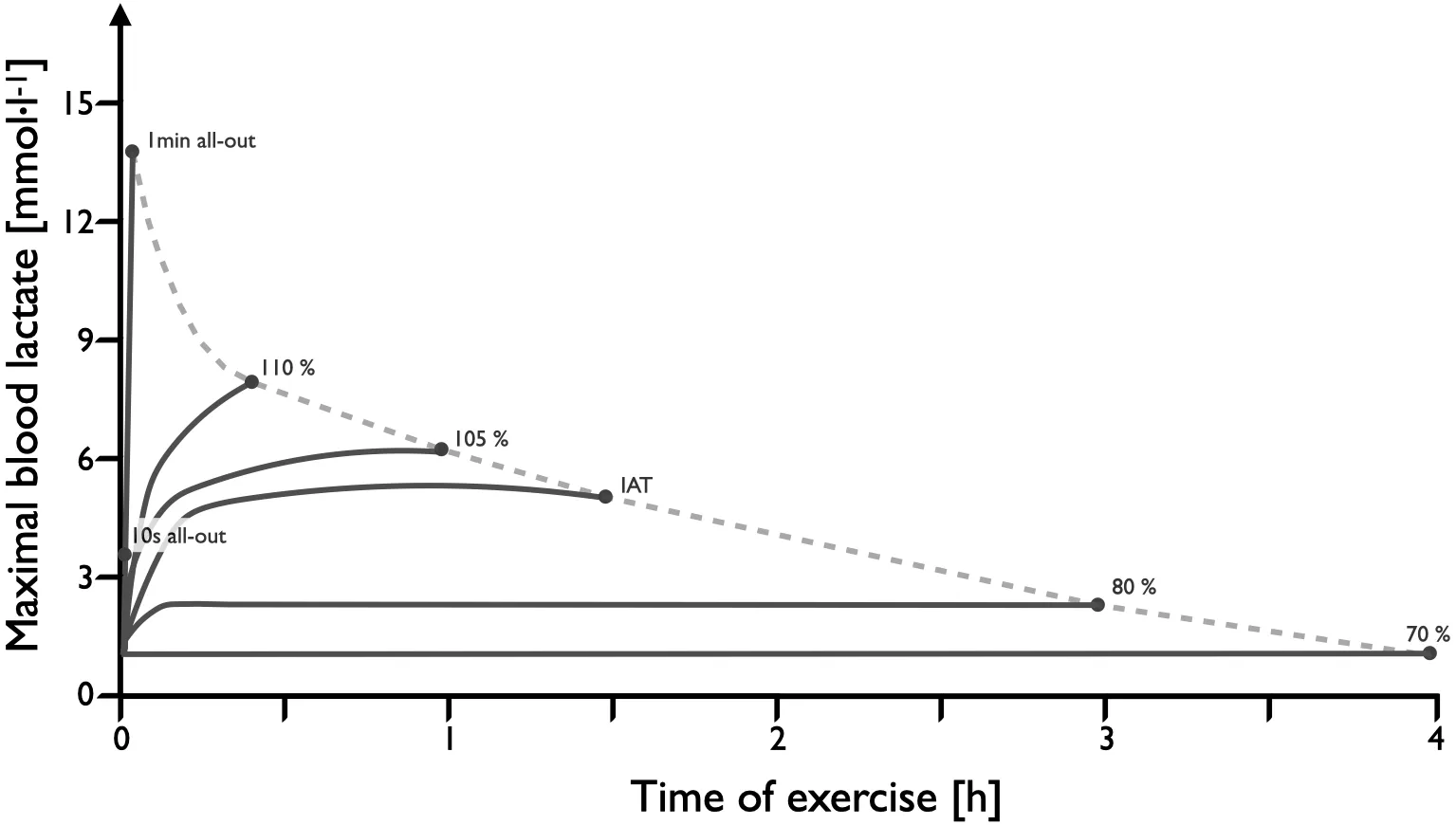
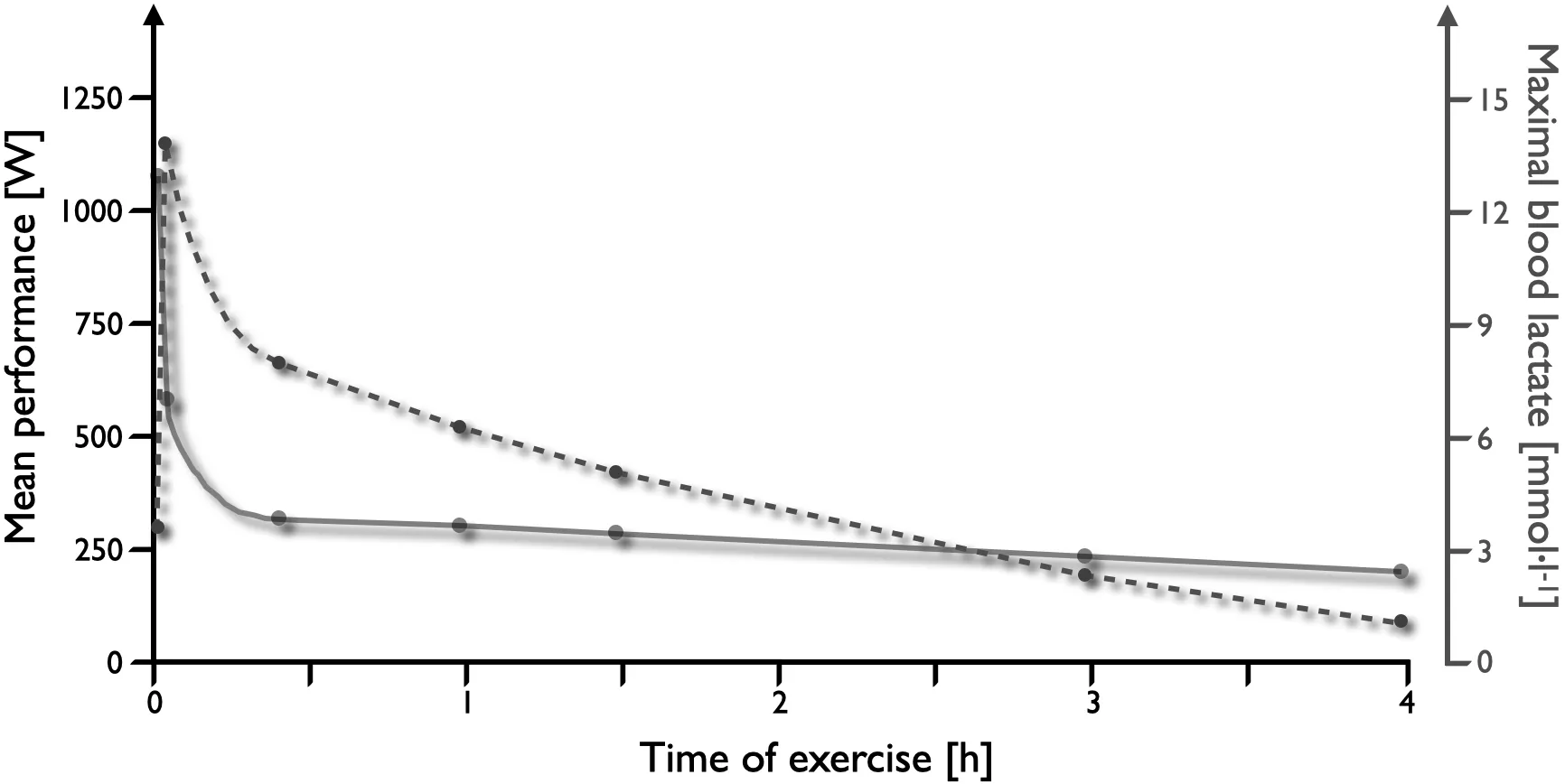
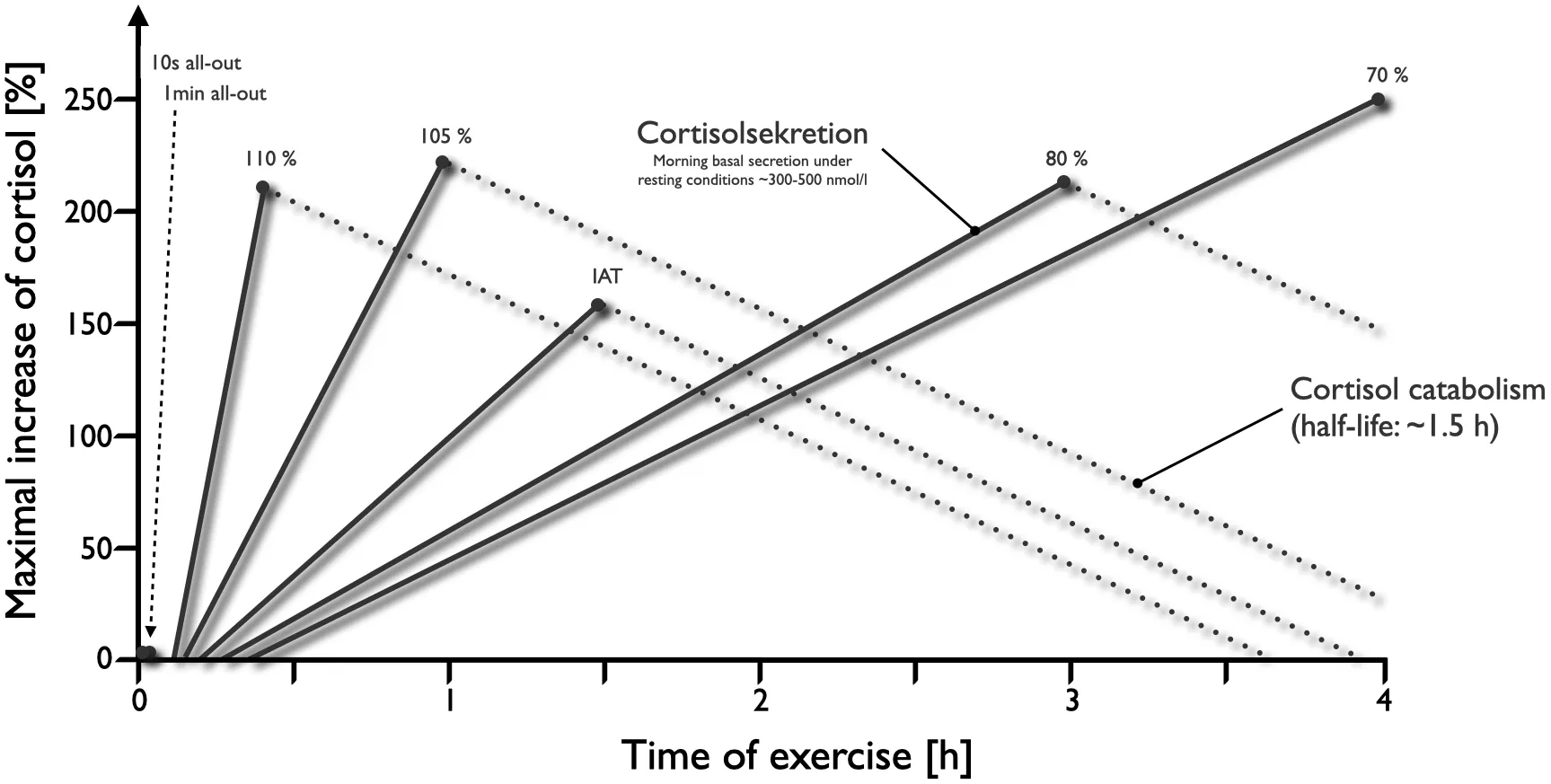
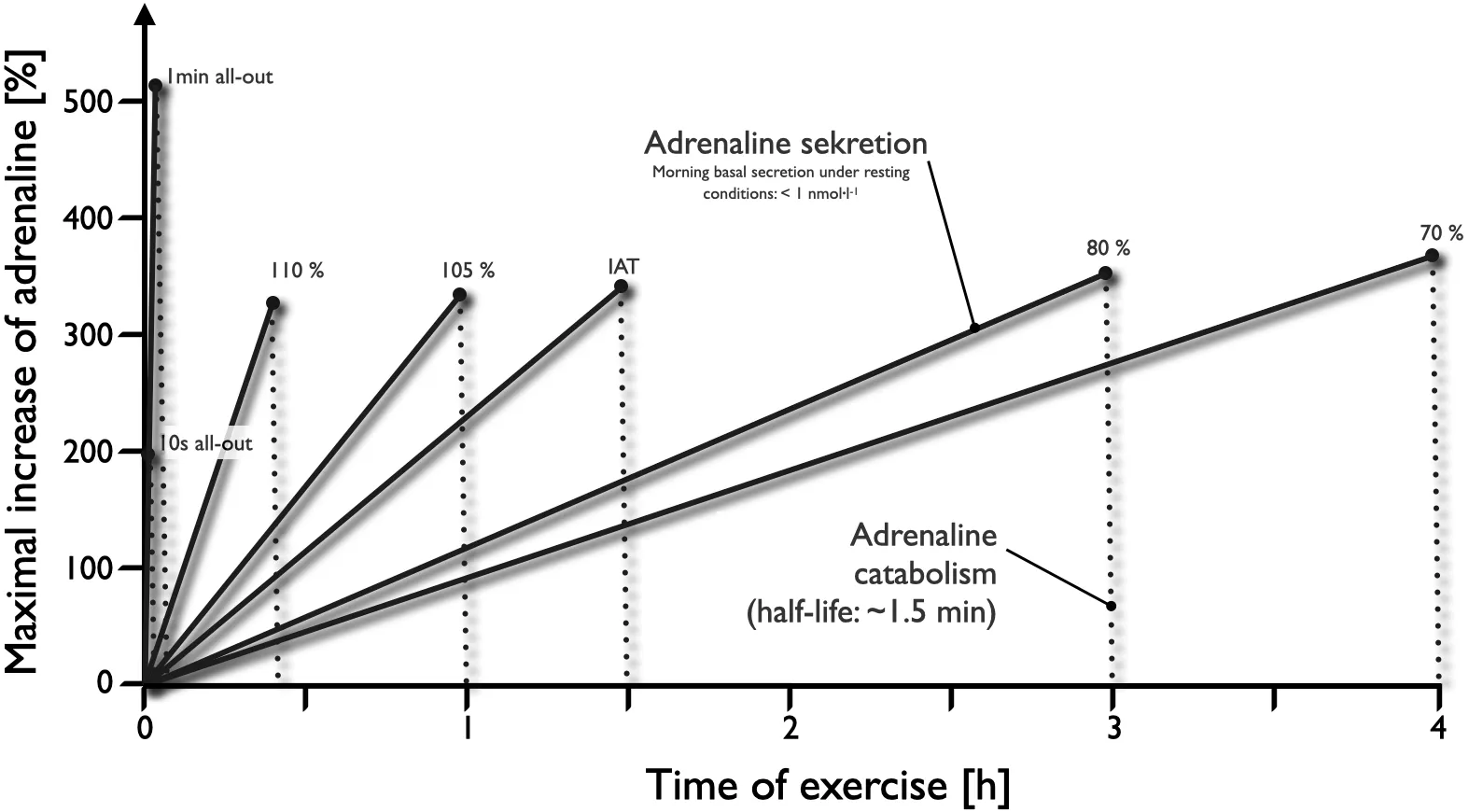
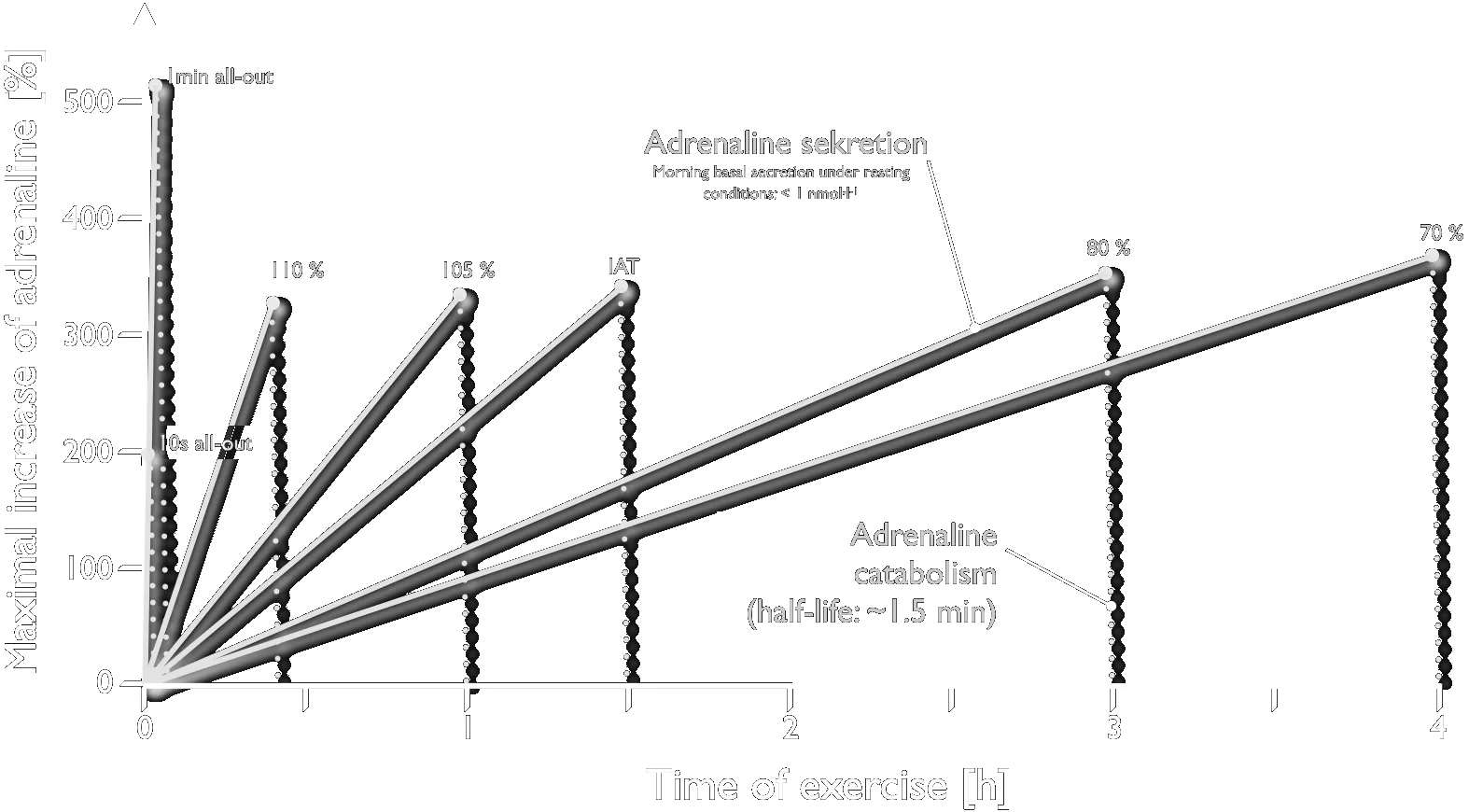
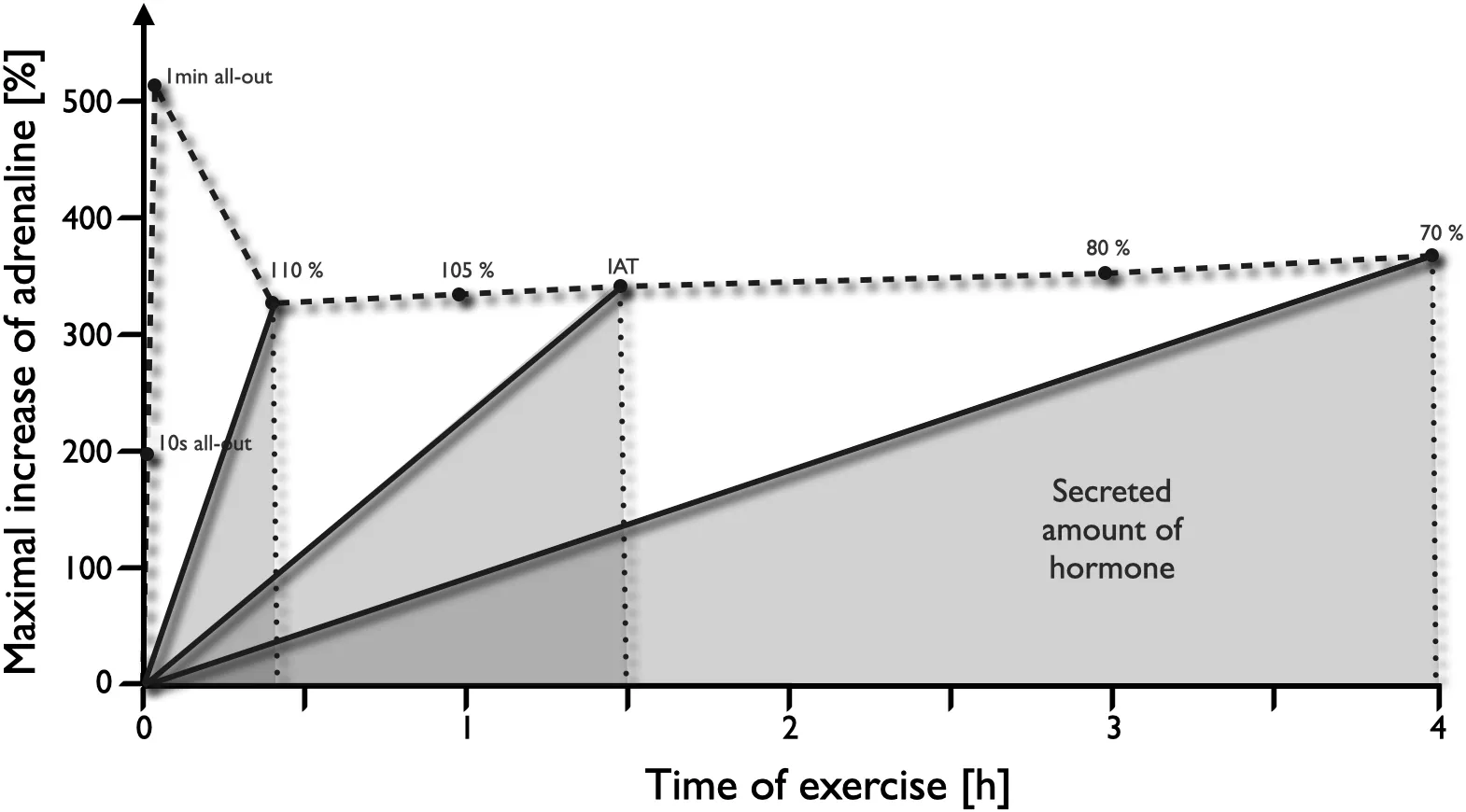
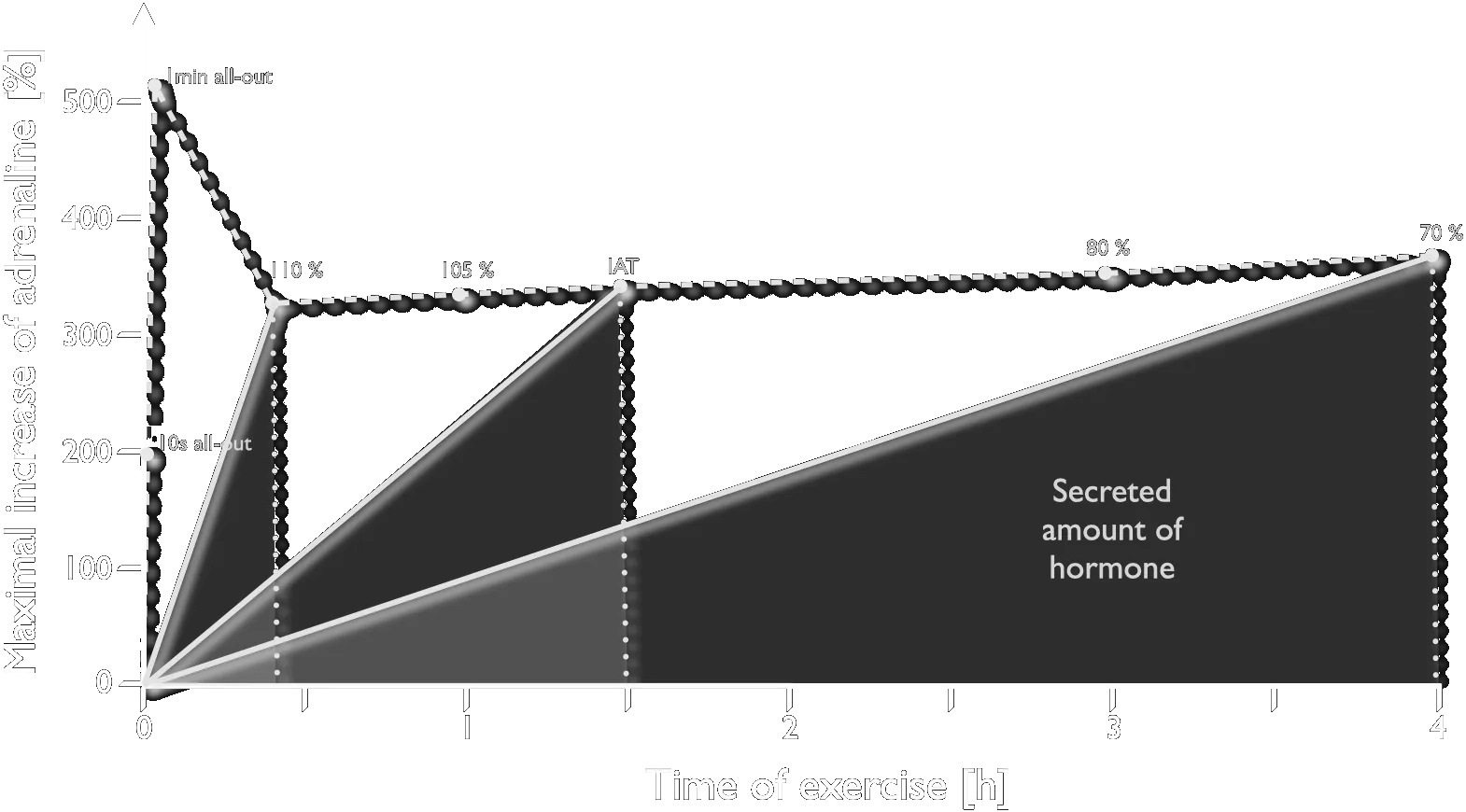
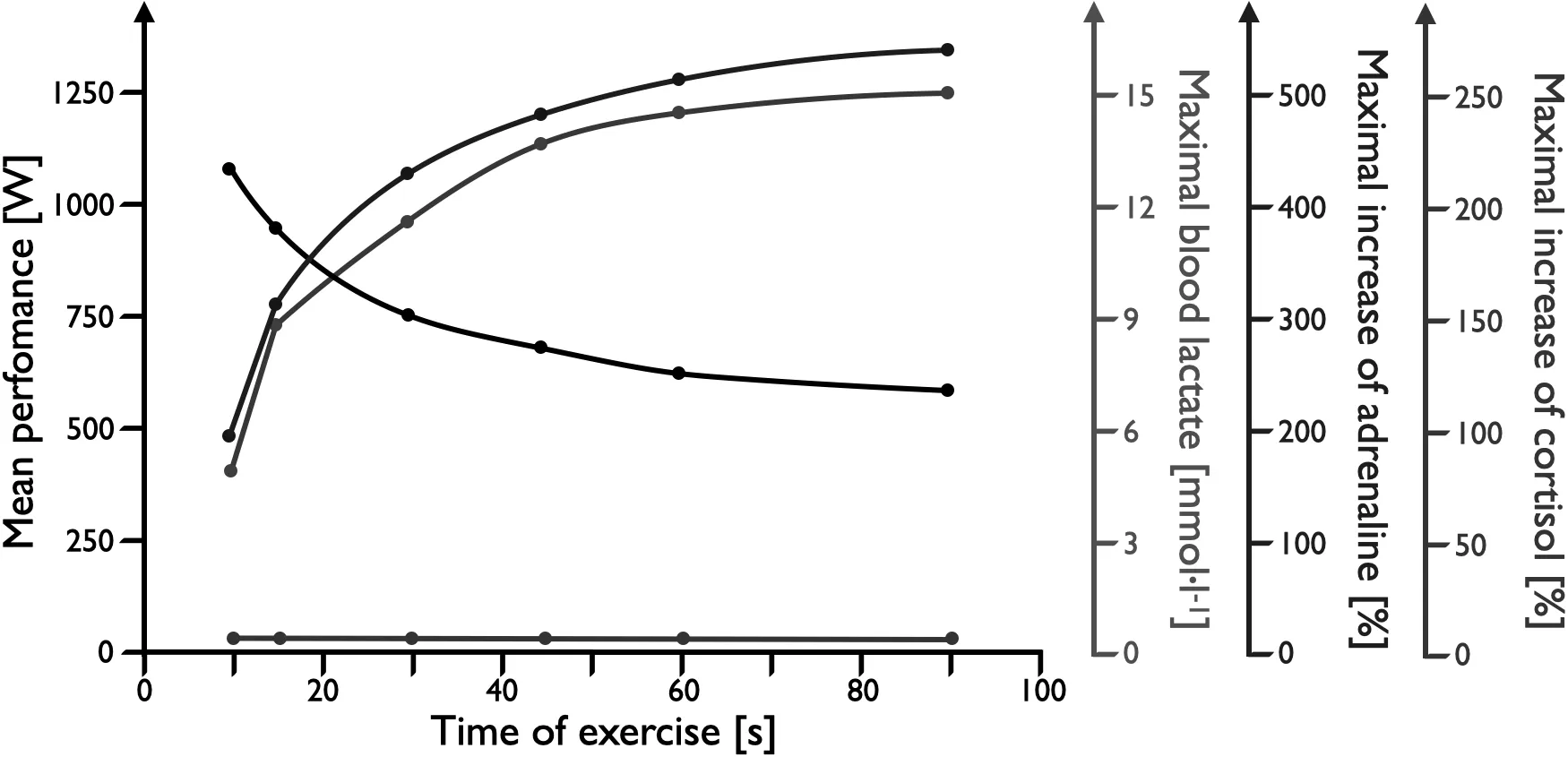
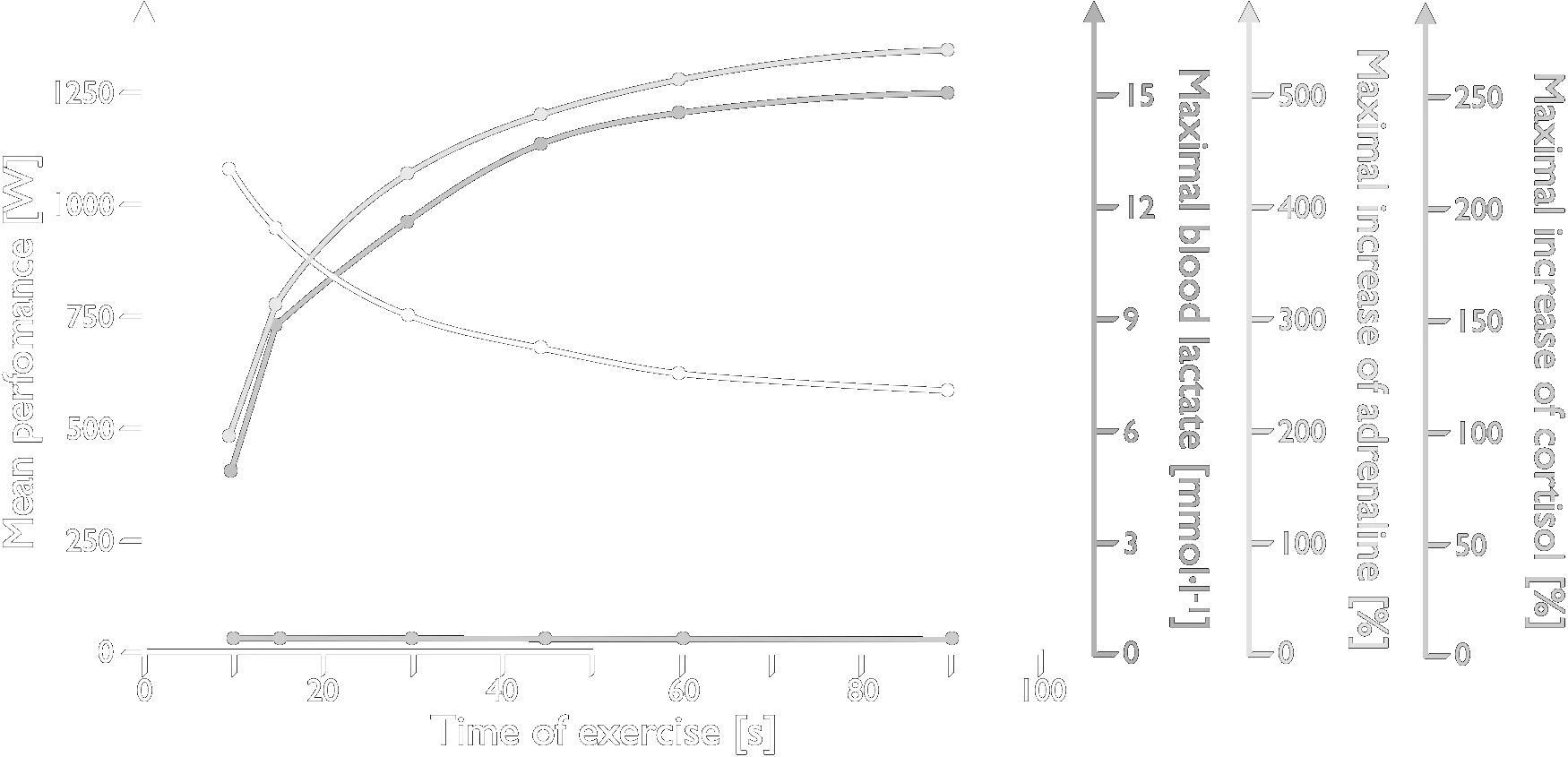
Cycle-ergometer exercise of different intensities and durations, showing performance, lactate generation and hormone secretion built up step by step. Male subjects with a V̇O₂max of 60–65 ml·min⁻¹·kg⁻¹.
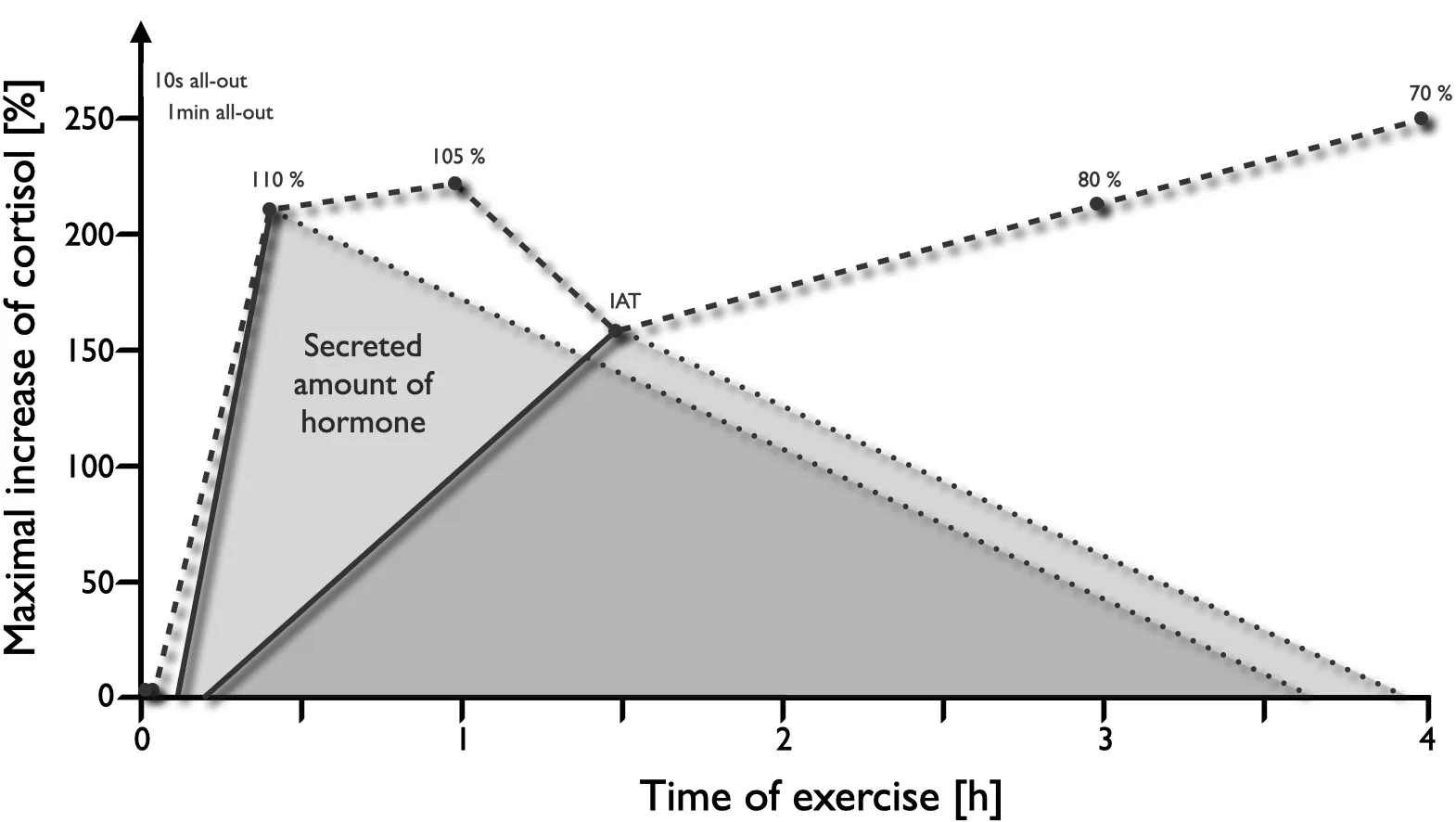
Overview of hormonal regulation and energy supply at different loads and load durations. RPE — rating of perceived exertion (Borg scale value).
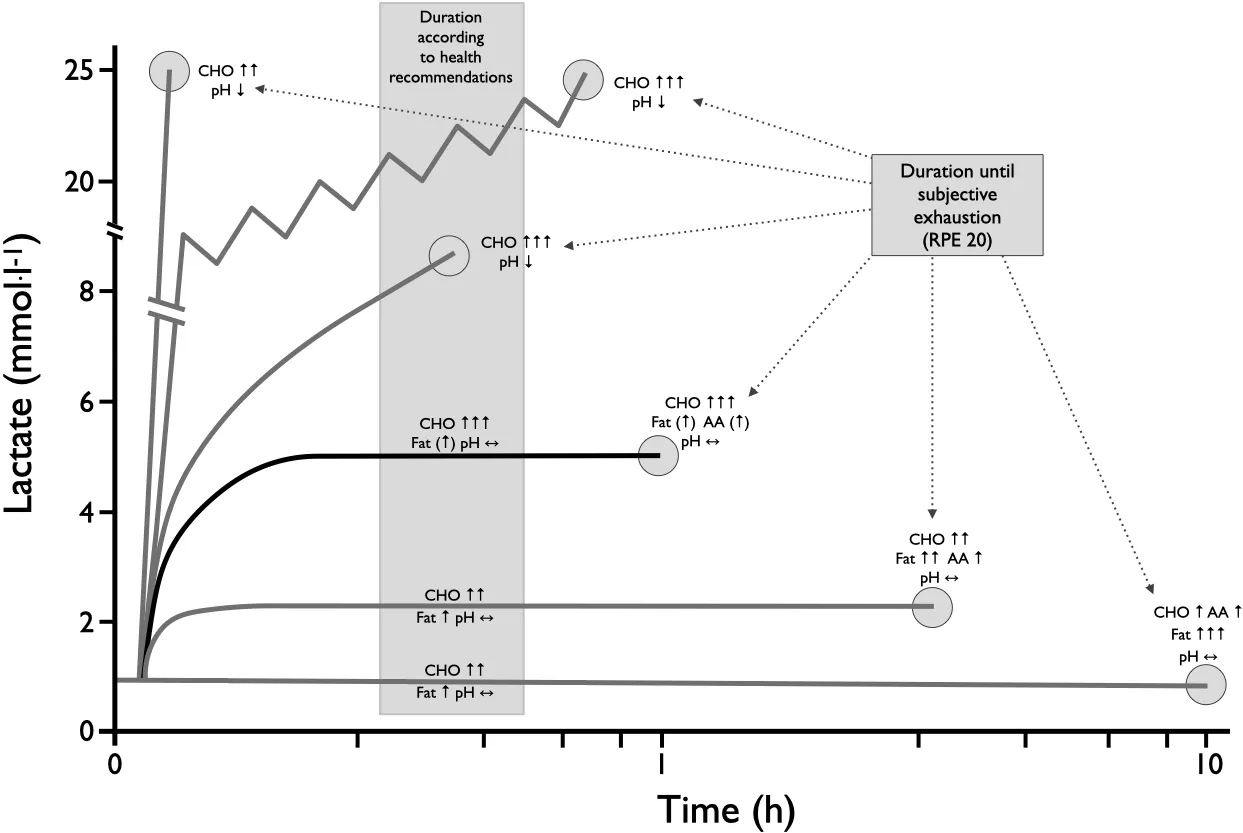
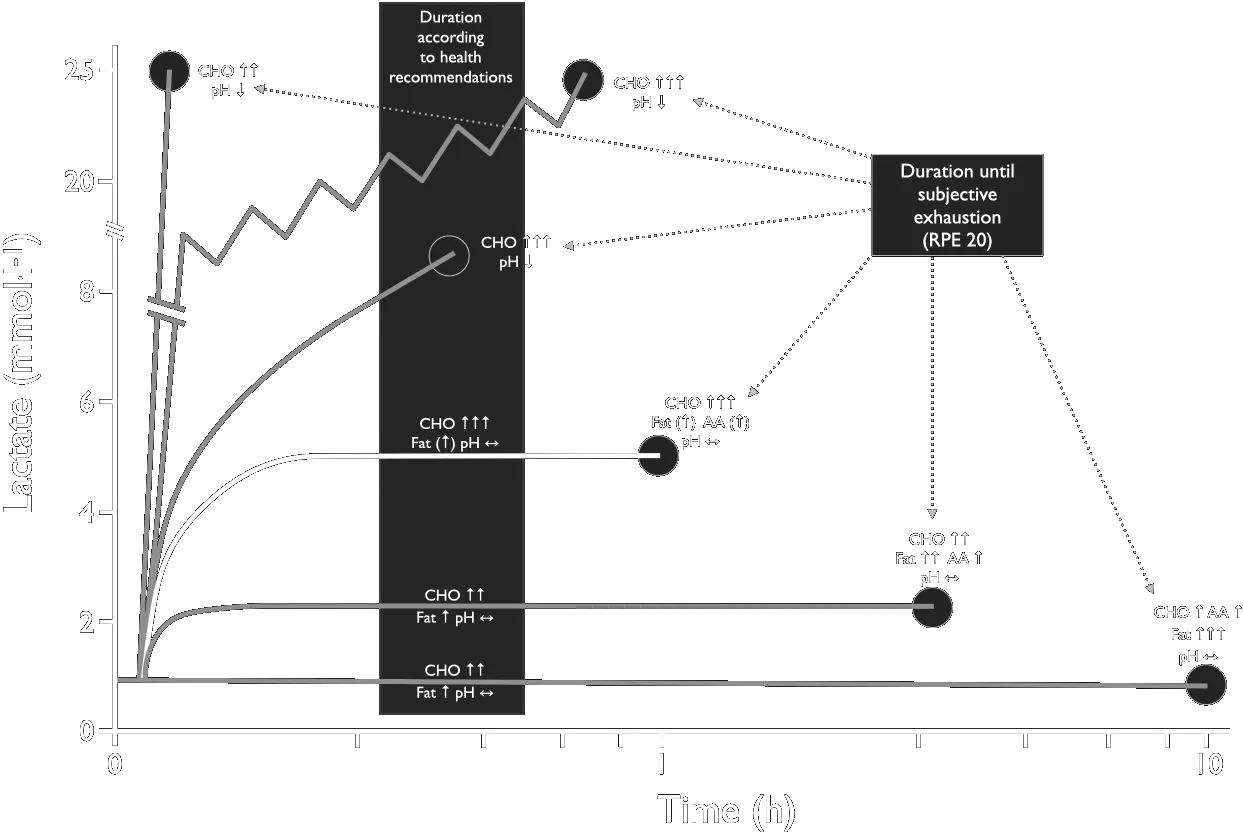
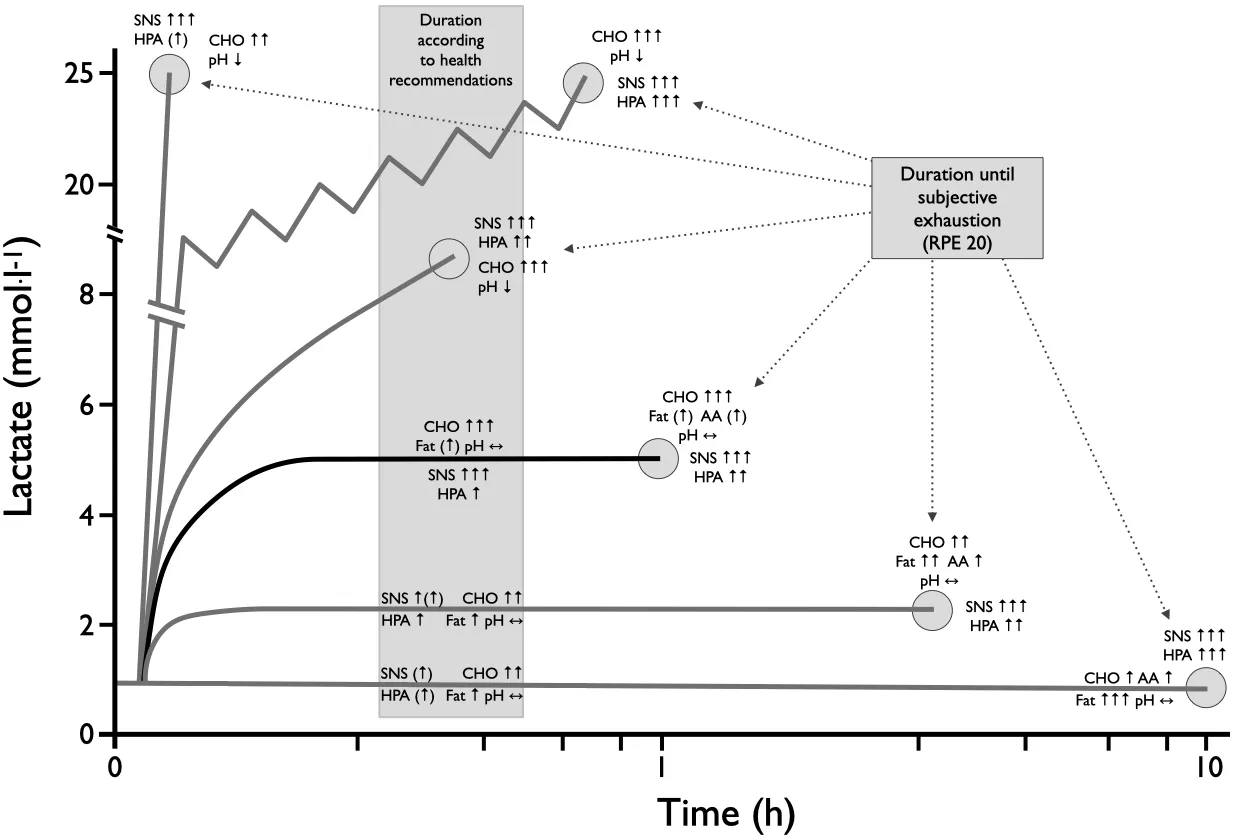
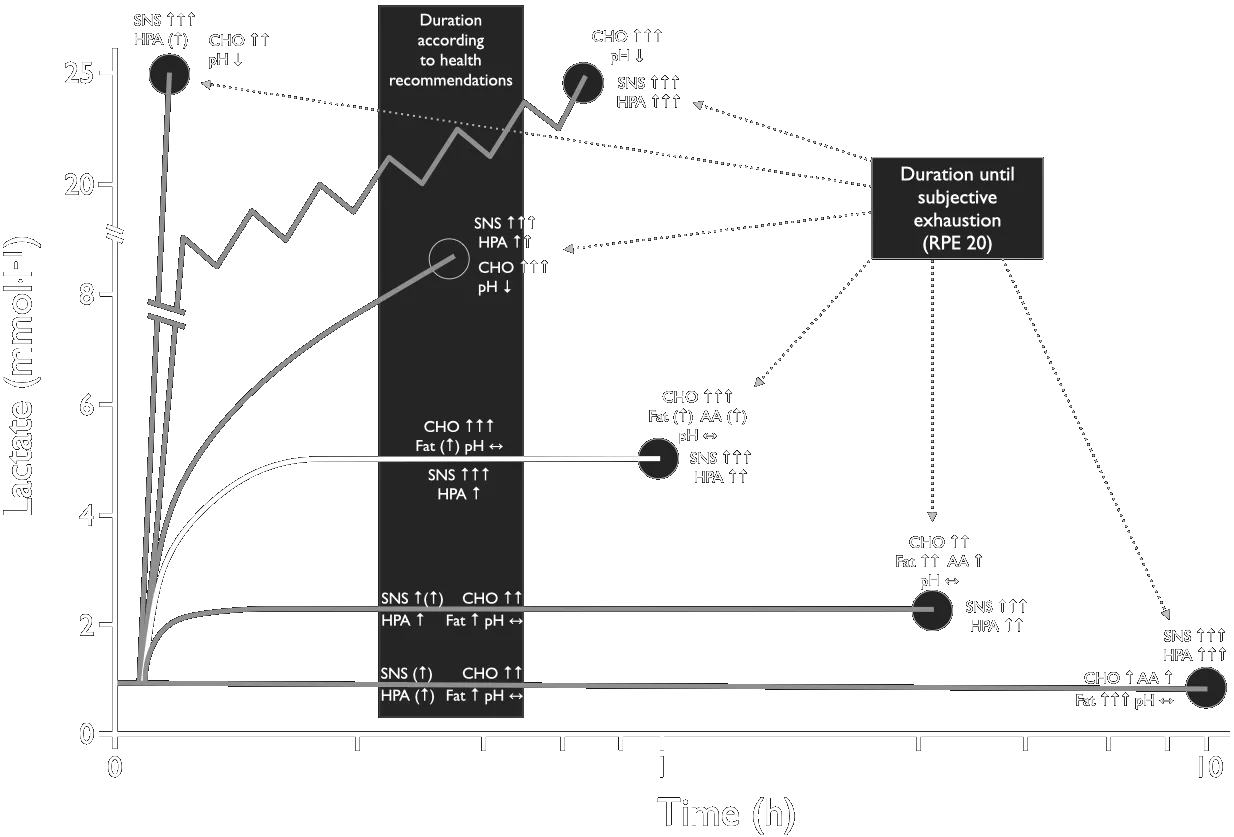
Overview of hormonal regulation and energy supply at different loads and load durations. RPE — rating of perceived exertion (Borg scale value).
3 Energy Balance
3.1 What Is Energy and What Is It For?
Each of the approximately 80 trillion (80·10¹²) cells in the human body requires energy to maintain structure and function. The key principle of homeostasis allows the energy supplied by food to be used for physiological work.
In the physiological sense, energy is synonymous with the supply and consumption of ATP.
High-energy phosphates, especially adenosine triphosphate (ATP), are the “currency” of energy — for example to perform mechanical muscle work. The task of the physiological regulatory systems is to provide the required amount of ATP at the right place, time and speed. ATP enables muscle tone during physical rest as well as fast and powerful contractions of the skeletal muscles. ATP can be made available under aerobic and anaerobic conditions for both slow and fast physical activity.
Energy exists in either potential or kinetic form. Potential energy refers to energy associated with a substance’s structure or position; kinetic energy refers to energy of motion. The six forms of energy are chemical, mechanical, heat, light, electrical, and nuclear — each can convert to another form.
- Exergonic reactions release energy to the surroundings.
- Endergonic reactions store, conserve, or increase free energy.
- Entropy describes the tendency of potential energy to degrade to kinetic energy with a lower capacity for work.
Enzymes represent highly specific protein catalysts that accelerate chemical reaction rates without being consumed. Coenzymes consist of nonprotein organic substances that facilitate enzyme action. Hydrolysis (catabolism) breaks down complex molecules; condensation (anabolism) synthesises complex biomolecules.
The transport of electrons by specific carrier molecules constitutes the respiratory chain — the final common pathway in aerobic metabolism.
3.2 How Does Energy Get Into the Organism?
Carbon, hydrogen, oxygen, and nitrogen represent the basic structural units for most of the body’s bioactive substances. Less than 40 % of food energy is available as utilisable or stored energy (net available energy, energy-rich phosphates) for skeletal muscle work.
Gross energy values (physical calorific values):
Physical (gross) and physiological energy values of the macronutrients, glucose and ethanol.
| Nutrient | Physical energy value (kcal·g⁻¹) | Physical energy value (kJ·g⁻¹) | Physiological energy value (kcal·g⁻¹) |
|---|---|---|---|
| Fat | 9.3 | 38.9 | 9.3 |
| Protein | 5.5 | 23.0 | 4.1 |
| Carbohydrate | 4.1 | 17.2 | 4.1 |
| Glucose | 3.8 | 15.7 | 3.8 |
| Ethanol | 7.1 | 29.7 | 7.1 |
Physical (gross) and physiological energy values of the macronutrients, glucose and ethanol.
Coefficients of digestibility average 97 % for carbohydrates, 95 % for lipids, and 92 % for proteins. The complete breakdown of 1 mole of glucose liberates 689 kcal of energy; of this, approximately 34 % is conserved in ATP bonds.
Energy transfer pathway:
- Complete oxidation of a glucose molecule in skeletal muscle yields a net gain of 32 ATP molecules.
- The complete oxidation of a triacylglycerol molecule yields approximately 460 ATP molecules.
- During intense exercise when hydrogen oxidation fails to keep pace with its production, pyruvate temporarily binds hydrogen to form lactate, allowing continuation of anaerobic glycolysis.
Energy intake and expenditure must be in balance. Any physical activity consumes energy. Even in an apparently inactive state, the organism needs energy. Physical activity strains the organism — the type and extent of the strain of cells, tissues and organs depends on type, duration, intensity and physiological functional status.
3.3 Energy Transfer — Macronutrients
3.3.1 Carbohydrates
Three major classifications: monosaccharides (glucose, fructose), oligosaccharides (sucrose, lactose, maltose), and polysaccharides (starch, fibre, glycogen). Carbohydrate serves four important functions: (1) major energy source; (2) spares protein breakdown; (3) metabolic primer for fat catabolism; (4) required fuel for the CNS.
Muscle glycogen provides the primary energy substrate during anaerobic exercise. A carbohydrate-deficient diet quickly depletes muscle and liver glycogen, profoundly affecting both all-out exercise capacity and sustained intense aerobic exercise. Individuals who train intensely should consume 60–70 % of daily calories as carbohydrates (400–800 g; 8–10 g·kg⁻¹ body mass).
3.3.2 Lipids
Lipids contain carbon, hydrogen, and oxygen but with a higher ratio of hydrogen to oxygen. Lipids provide the largest nutrient store of potential energy for biological work. Fat contributes 50–70 % of the energy requirement during light- and moderate-intensity physical activity. Stored intramuscular fat and fat derived from adipocytes become important during prolonged exercise, supplying more than 80 % of exercise energy requirements.
Saturated fatty acids exist primarily in animal meat, egg yolk, dairy fats, and cheese — elevated intake promotes coronary heart disease. Unsaturated fatty acids protect against coronary heart disease. Aerobic training increases long-chain fatty acid oxidation during mild-to-moderate intensity exercise.
3.3.3 Proteins
Proteins differ from lipids and carbohydrates because they contain nitrogen in addition to sulfur, phosphorus, and iron. The body requires 20 different amino acids; 8 are essential and must be consumed in the diet. The Recommended Dietary Allowance (RDA) for protein in adults equals 0.83 g·kg⁻¹ body mass. For athletes engaged in intense training, increasing protein intake to 1.2–1.8 g·kg⁻¹ body mass daily is reasonable.
The muscle-derived amino acid alanine plays a key role via gluconeogenesis in supporting carbohydrate availability during prolonged exercise (alanine–glucose cycle accounts for up to 45 % of the liver’s glucose release during long-duration exercise).
References
- [1] Gabriel H. Bewegung, Leistungsfähigkeit und Aktivität des Menschen. Gestaltungsmöglichkeiten und Grenzen aus physiologischer, sportmedizinischer und gesundheitsförderlicher Perspektive. In Religion und Bildung — Ressourcen im Alter?, pp. 19–40. Beier, Miriam and Gabriel, Holger and Rieger, Hans-Martin and Wermke Michael, 2016.
- [2] Brixius K. Sport und Leistungsphysiologie. In Brandes R, Lang F, Schmidt RF (eds): Physiologie des Menschen mit Pathophysiologie, chapter 44, pp. 561–579. Springer-Verlag, 32. Auflage, 2019. https://doi.org/10.1007/978-3-662-56468-4
One-Minute-Paper Topics
A One-Minute-Paper (OMP) is a short, focused prompt that students answer in ~60 seconds at the end of a session to consolidate learning, surface misconceptions, and provide formative feedback. When answering, be concise, specific, and use terminology from today’s session.
- In one sentence, what is the central function of the immune system in the context of “bodily integrity”?
- Distinguish innate from adaptive immunity using one cell type and one mechanism for each.
- Why is acute inflammation considered a protective response while chronic inflammation is considered pathological?
- Give one example of how a single bout of moderate exercise transiently modulates immune cell trafficking.
- Explain the “open window” hypothesis and why it remains debated.
- How does habitual moderate exercise differ from prolonged strenuous exercise in its effect on immune function?
- Define “limits of performance” from a physiological perspective and name one limiting system.
- How does ageing alter the determinants of physical performance capacity?
- Why is age-related mortality risk now included in extended definitions of physical performance?
- State the first law of thermodynamics applied to human energy balance in one sentence.
- Why is energy balance better described as a dynamic equilibrium than a static equation?
- Compare the ATP yield per gram of carbohydrate, lipid, and protein and note one reason fats yield more.
- Outline one entry point at which carbohydrates feed into ATP production during exercise.
- Why is lipid oxidation favoured at lower exercise intensities?
- Under what conditions does protein become a meaningful energy substrate during exercise?
- Describe one hormonal signal that links nutrient intake to energy utilisation during exercise.
- How might chronic energy deficiency (e.g., RED-S) affect both immune function and performance?
- Give one practical reason why understanding immune-exercise interactions matters for clinical populations such as Long COVID patients.
- Which limit of performance do you think is most underestimated by recreational athletes, and why?
- What concept from today’s lecture would you most like to see illustrated with real data next time?