Protein Intake in Sport - How Much Is Appropriate?
Table of Contents
- What Drives the “Protein Obsession”?
- What Recommendations Exist?
- Protein Intake in Athletes
- Safety Concerns and High Protein Intake
- Summary
What Drives the “Protein Obsession”?
A 2024 annual survey published by the International Food Information Council among US Americans revealed that 71% wished to increase their protein intake — more than for any other dietary component. In 2022, this figure for protein was 52% [1]. A survey among non-professional athletes who use protein supplements found that 40% of these individuals obtain their information on protein supplementation from social media [2]. This growing interest in protein reflects broader nutritional trends and underscores the potentially perceived benefits for health and fitness [3].
What Recommendations Exist?
The recommended daily protein intake is 0.8 g·kg⁻¹·day⁻¹, corresponding to approximately 11% of total energy requirements [4, 5, 6]. On average, individuals in Western societies consume approximately one-third more protein than the recommended daily intake, and roughly one-quarter of the population consumes more than double the recommended amount (i.e., more than 1.6 g·kg⁻¹·day⁻¹ or 22% of daily energy intake in the form of protein) [6]. This trend raises questions regarding the long-term health effects of high-protein diets.
Protein Intake in Athletes
Recommendations for protein intake are among the most common and detailed nutrient recommendations. They encompass daily intake patterns, training-related intake, protein types, total daily intake, as well as portion sizes and timing of consumption [7]. Sport-specific and exercise-dependent protein intake can effectively support the training process and enhance performance. Currently, a protein intake of approximately 1.2 to 2.0 grams per kilogram of body weight is recommended for athletes, depending on training status and training goals [8]. Athletes often require higher protein amounts, typically between 1.2 and 2.0 g/kg/day, to promote muscle repair and muscle growth while simultaneously minimizing the risk of muscle loss during periods of intense training [9]. Protein intake should not be considered a fixed parameter in athletes’ nutrition plans but can be flexibly adjusted to training goals, intensity, and volume. Due to the longer metabolic window for protein synthesis compared to carbohydrates, protein should be consumed multiple times daily (3–4 times/day).
General Evidence (Consensus and Review Papers)
- General: ~1.2–2.2 g/kg/day as the appropriate range for most athletes
- Daily intake during short-term intensive training: 1.2–2.0 g/kg/day
- Endurance: ~1.2–1.5 g/kg/day (including recovery)
- Strength/Power: ~1.6–1.8 g/kg/day (to maximize training adaptations)
- Post-exercise: 0.4 g/kg/day (combined with 0.8 g/kg carbohydrates for targeted muscle glycogen recovery)
- Injury: 1.6–2.0 g/kg/day (depending on the type of injury)
Recommended daily protein intake by body weight and exercise type. Puta C (2025), based on Egan, B. Nutr. Bull. 41, 202–213 (2016). Delany, L. V., Costello, N., Jones, B. & Backhouse, S. H. Sports Med. 55, 2445–2487 (2025). Jäger, R. et al. . J. Int. Soc. Sports Nutr. 14, 20 (2017).
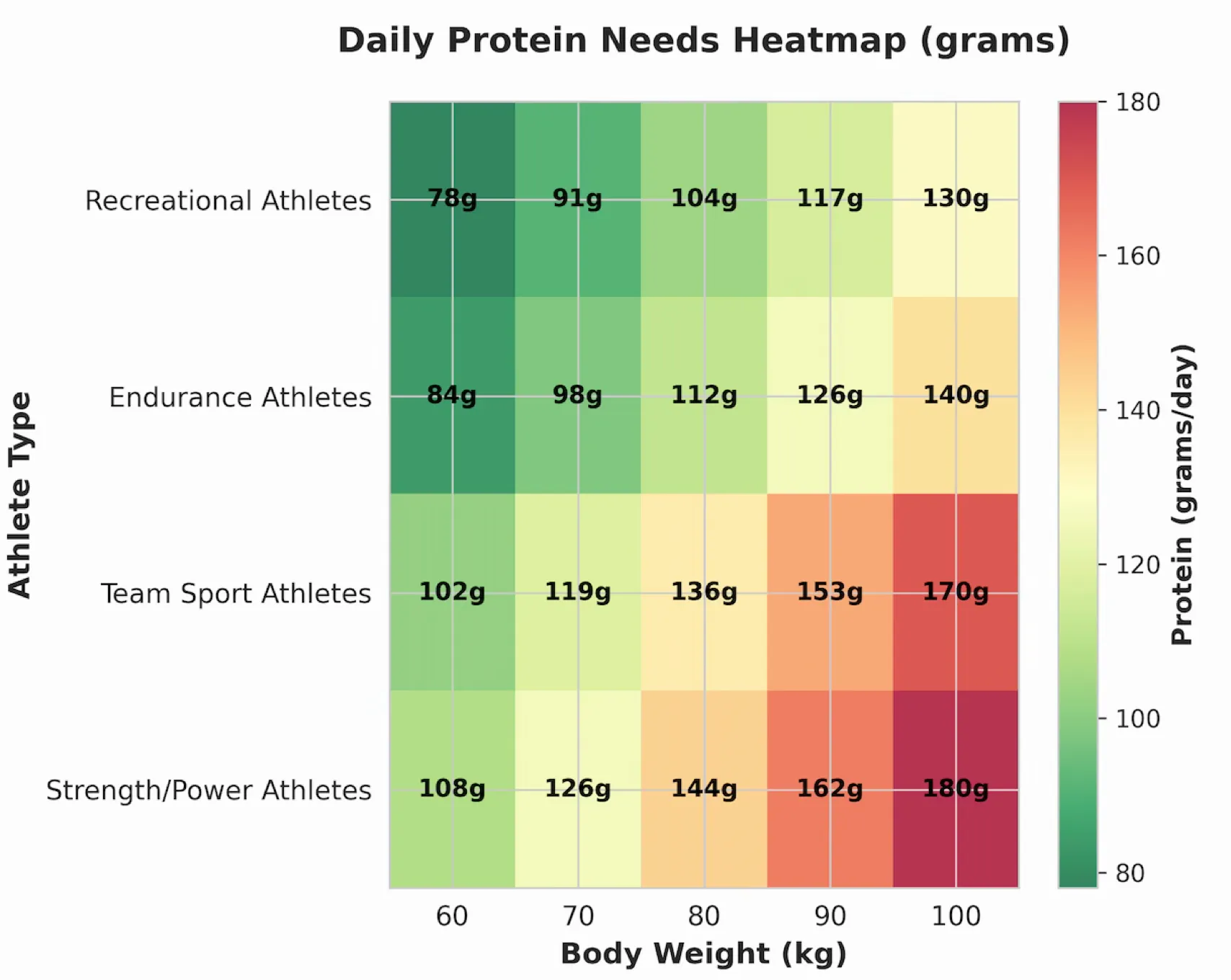
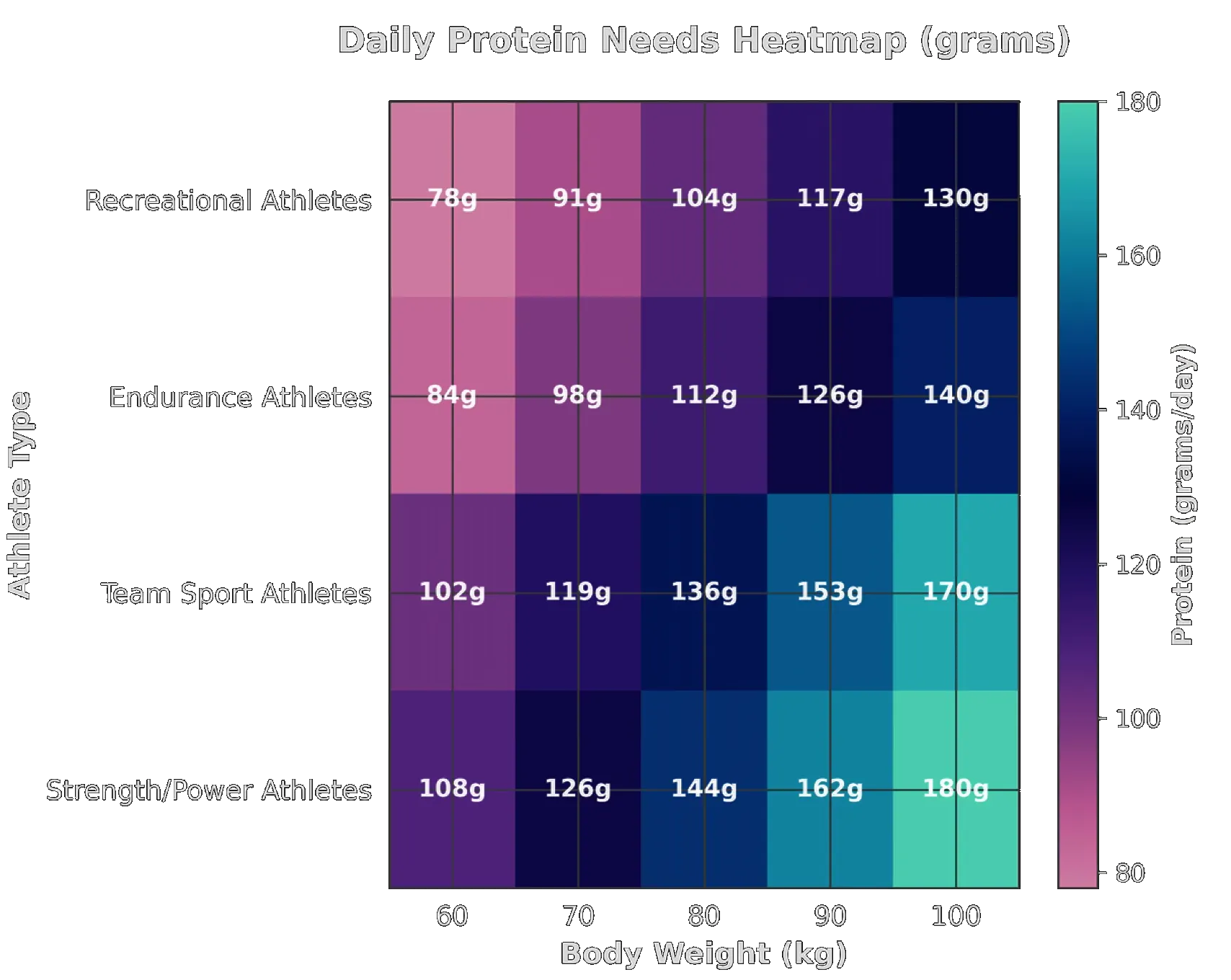
Recommended daily protein intake by body weight and exercise type. Puta C (2025), based on Egan, B. Nutr. Bull. 41, 202–213 (2016). Delany, L. V., Costello, N., Jones, B. & Backhouse, S. H. Sports Med. 55, 2445–2487 (2025). Jäger, R. et al. . J. Int. Soc. Sports Nutr. 14, 20 (2017).
What is the principal driver for building muscle mass and strength? Puta C (2025), based on Egan, B. Nutr. Bull. 41, 202–213 (2016). Delany, L. V., Costello, N., Jones, B. & Backhouse, S. H. Sports Med. 55, 2445–2487 (2025). Jäger, R. et al. . J. Int. Soc. Sports Nutr. 14, 20 (2017).
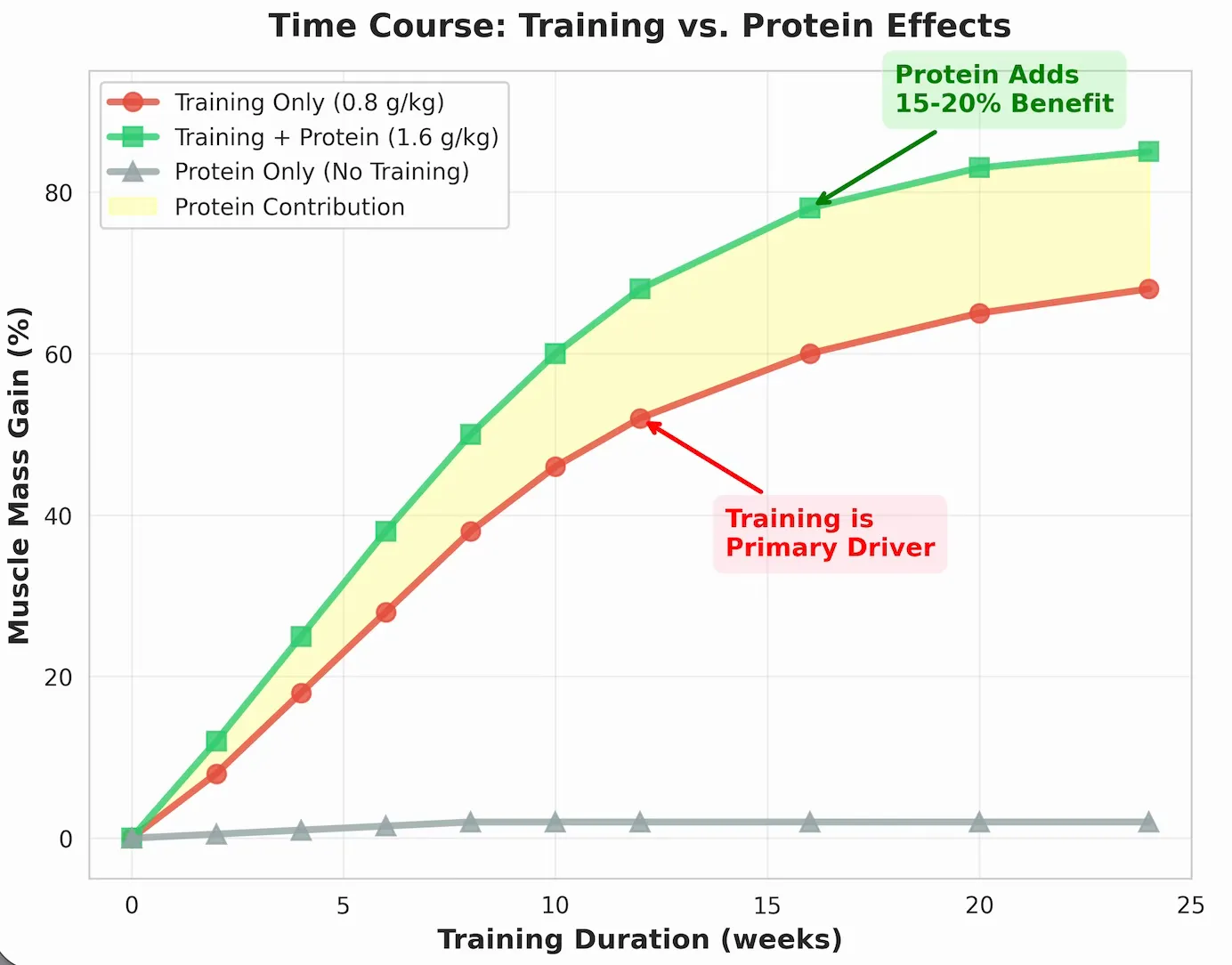
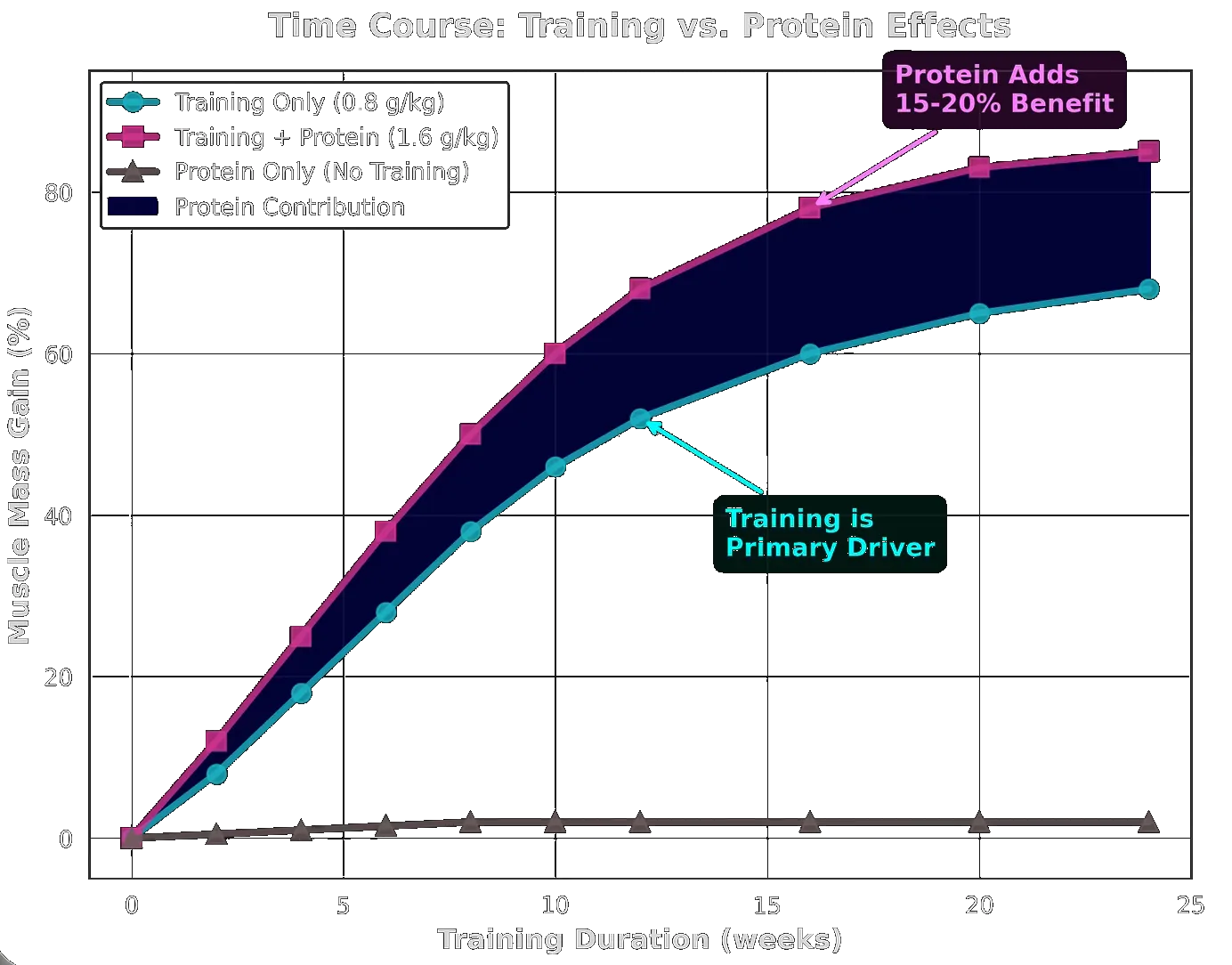
What is the principal driver for building muscle mass and strength? Puta C (2025), based on Egan, B. Nutr. Bull. 41, 202–213 (2016). Delany, L. V., Costello, N., Jones, B. & Backhouse, S. H. Sports Med. 55, 2445–2487 (2025). Jäger, R. et al. . J. Int. Soc. Sports Nutr. 14, 20 (2017).
Safety Concerns and High Protein Intake
A high protein intake exceeding 1.5 g/kg/day has been shown to activate the mammalian target of rapamycin (mTOR) in macrophages (via elevated leucine levels), thereby promoting atherosclerosis progression through inhibition of damaged mitochondrial clearance (mitophagy) [6, 10]. This suggests that while protein is essential for recovery and performance, excessive intake may exert adverse effects on cardio-metabolic processes. Notably, the identified threshold of dietary leucine-activated mTORC1 signaling in macrophages appears to coincide with the maximal stimulatory effect of dietary protein on muscle protein synthesis at approximately 25–30 g per meal. This implies a complex, integrated metabolic network of multi-organ physiological functions that ensures optimal health [6]. Therefore, while protein is of critical importance for athletes, careful consideration of intake is necessary to balance performance benefits against potential health risks.
Summary
The available scientific evidence on protein intake does not support very high protein consumption, particularly not substantially exceeding approximately 1.6 g/kg/day, which corresponds to roughly double the recommended daily allowance. No high-quality data (e.g., randomized controlled trials, meta-analyses) exist to support the recommendation of approximately triple the recommended daily allowance, as advocated by proponents of very high protein intake. An intake of 1.5 to 2 times the recommended daily allowance may be beneficial for athletes and individuals engaging in regular physical activity. In summary, while protein is indispensable for athletic performance, excessive intake beyond recommended amounts may pose health risks. Therefore, a balanced approach to dietary protein intake is warranted.
References
[1] International Food Information Council. 2024 Food & Health Survey. Available at: https://ific.org/wp-content/uploads/2024/06/2024-IFIC-Food-Health-Survey.pdf
[2] MDPI Dietetics 2024; 5(2):18. Available at: https://www.mdpi.com/2673-9488/5/2/18
[3] The New York Times. The Daily Podcast: Protein Bars America. 2025 Aug 26. Available at: https://www.nytimes.com/2025/08/26/podcasts/the-daily/protein-bars-america.html
[4] Deutsche Gesellschaft für Ernährung (DGE). Referenzwerte Protein. Available at: https://www.dge.de/wissenschaft/referenzwerte/protein/
[5] National Academies of Sciences, Engineering, and Medicine. Dietary Reference Intakes for Energy, Carbohydrate, Fiber, Fat, Fatty Acids, Cholesterol, Protein, and Amino Acids. Washington, DC: The National Academies Press. Available at: https://nap.nationalacademies.org/read/11537/chapter/14
[6] Zhang X, Kapoor D, Jeong SJ, Fappi A, Stitham J, Shabrish V, Sergin I, Yousif E, Rodriguez-Velez A, Yeh YS, Park A, Yurdagul A Jr, Rom O, Epelman S, Schilling JD, Sardiello M, Diwan A, Cho J, Stitziel NO, Javaheri A, Lodhi IJ, Mittendorfer B, Razani B. Identification of a leucine-mediated threshold effect governing macrophage mTOR signalling and cardiovascular risk. Nat Metab. 2024 Feb;6(2):359–377. doi: 10.1038/s42255-024-00984-2. PMID: 38409323; PMCID: PMC11448845.
[7] Delany LV, Costello N, Jones B, Backhouse SH. Dietary Recommendations for Body Mass and Composition Manipulation in Male and Female Athletes: a Scoping Review of Consensus Statements, Position Stands and Practice Guidelines from International Expert Groups. Sports Med. 2025 Oct;55(10):2445–2487. doi: 10.1007/s40279-025-02285-4. PMID: 40841871; PMCID: PMC12513969.
[8] König D, Carlsohn A, Braun H, Großhauser M, Lampen A, Mosler S, Nieß A, Schäbethal K, Schek A, Virmani K, Ziegenhagen R, Heseker H. Protein Intake in Sport. Position of the Working Group Sports Nutrition of the German Nutrition Society (DGE). Ernährungs Umschau International. 2020;7/2020.
[9] Egan B. Protein Intake for Athletes and Active Adults: Current Concepts and Controversies. Nutr Bull. 2016;41:202–213. doi: 10.1111/nbu.12215
[10] Mittendorfer B, Klein S, Fontana L. A word of caution against excessive protein intake. Nat Rev Endocrinol. 2020 Jan;16(1):59–66. doi: 10.1038/s41574-019-0274-7. PMID: 31728051.
One-Minute-Paper Topics
A One-Minute-Paper (OMP) is a short, focused prompt that students answer in ~60 seconds at the end of a session to consolidate learning, surface misconceptions, and provide formative feedback. When answering, be concise, specific, and use terminology from today’s session.
- A 2024 IFIC survey found that 71% of US Americans wanted to increase protein intake — the highest of any nutrient. What social and media factors drive this trend, and how should a sports scientist respond when a non-athlete asks whether they need more protein?
- The recommended daily allowance for protein in the general adult population is 0.8 g·kg⁻¹·day⁻¹ (~11% of total energy). On what type of evidence is this recommendation based, and what does it define — minimum sufficiency or optimal intake?
- On average, people in Western societies consume about one-third more protein than the RDA, and roughly one-quarter consume more than double the RDA (>1.6 g·kg⁻¹·day⁻¹). What concerns does this widespread over-consumption raise for long-term health?
- Why do athletes require more protein than the general population RDA? Describe the two main physiological purposes (muscle repair and muscle growth vs. prevention of muscle loss during intense training) and explain why this range varies across sport types.
- Compare the recommended daily protein intakes for endurance athletes (~1.2–1.5 g·kg⁻¹) and strength/power athletes (~1.6–1.8 g·kg⁻¹). What is the physiological rationale for the difference?
- The lecture recommends 0.4 g·kg⁻¹ protein post-exercise combined with 0.8 g·kg⁻¹ carbohydrates for targeted muscle glycogen recovery. Explain the biochemical rationale: why is the co-ingestion of carbohydrates important for protein anabolic signalling?
- Why should protein be consumed 3–4 times per day rather than in one or two large boluses? What is the maximal per-meal stimulatory effect on muscle protein synthesis (~25–30 g), and why does exceeding this threshold not produce additional anabolic benefit?
- The lecture presents evidence that resistance training — not dietary protein per se — is the primary driver of muscle mass and strength gains. What is the practical implication of this for recreational athletes who focus on protein supplementation over training quality?
- High protein intake (>1.5 g·kg⁻¹·day⁻¹) activates mTOR in macrophages via elevated leucine, promoting atherosclerosis by inhibiting mitophagy. Describe this mechanism and explain why it implies a complex metabolic trade-off in high-protein diets.
- mTORC1 activation by dietary leucine suppresses mitophagy (clearance of damaged mitochondria) in macrophages. Why is impaired mitophagy in macrophages pro-atherogenic, and what does this mean for the optimal protein ceiling in high-performance athletes?
- A survey found that 40% of non-professional athletes who use protein supplements obtain their information from social media. What are the specific risks of this information source, and what are the key accuracy and safety concerns when social media meets sports nutrition?
- Injury-specific protein recommendations reach 1.6–2.0 g·kg⁻¹·day⁻¹. What physiological processes during healing justify this elevated intake? How should protein quality (essential amino acid profile, leucine content) be considered during injury recovery?
- The lecture states that protein intake “should not be a fixed parameter” but should be adjusted to training goals, intensity, and volume. Design a simple two-week periodisation example for a strength athlete alternating between high-volume and recovery weeks.
- Eight of the 20 amino acids are essential (cannot be synthesised by the body). Which essential amino acids are most critical for muscle protein synthesis after resistance exercise, and why does protein source (animal vs. plant) matter for their bioavailability?
- Protein deficiency impairs immune function by limiting lymphocyte proliferation, antibody synthesis, and cytokine production. At what intake level does protein become limiting for immune competence in athletes during heavy training, and how does this intersect with Relative Energy Deficiency in Sport (RED-S)?
- Muscle-derived amino acids (especially alanine) can contribute up to 45% of hepatic glucose release during prolonged exercise via gluconeogenesis. How does protein intake in the days prior to a long endurance event affect this contribution?
- Evaluate the evidence for three common protein supplement formats (whey protein, casein, plant-based protein blends). Under what circumstances does supplementation provide a measurable benefit beyond whole-food protein sources?
- High protein intake is often claimed to harm kidney function. What does the current evidence say for individuals with healthy kidneys vs. those with pre-existing renal disease? Where should the upper safety limit be set for otherwise healthy athletes?
- Anabolic resistance (reduced sensitivity of muscle protein synthesis to protein ingestion) increases with age. How should protein intake recommendations for masters athletes (>50 years) differ from those for younger athletes, and what is the recommended per-meal dose to overcome anabolic resistance?
- A 28-year-old recreational runner (70 kg, training 5 days/week, half-marathon goal) asks whether they need protein supplements. Using the evidence presented in this lecture, give a clear, evidence-based recommendation specifying: (a) target daily protein intake; (b) distribution across meals; (c) whether supplements are necessary; and (d) one safety consideration.