Basics in Exercise Physiology and Immunology - Key Concepts, Homeostasis and Hormesis
Table of Contents
- Key Terms of Physical Activity and Exercise
- Short-Term Balancing of Homeostasis
- Homeostasis and Hormesis
- From Homeostatic Regulation to Hormetic Adaptation
- Hormetic Stress Response
- The Dual Identity of Inflammatory Mediators
- Molecular Mediators of the Hormetic Response
- Biphasic Dose-Response and the J-Curve of Immune Function
- Complementary Temporal Scales
- Pathological Contexts: ME/CFS, Long COVID, and Post-Exertional Malaise
- State of Sleep and Wakefulness
- References
- One-Minute-Paper Topics
1 Key Terms of Physical Activity and Exercise in relation to Energy Expenditure and Metabolic Strain
Definition of Physical Activity
Physical activity, in the broadest sense, is every bodily movement performed by skeletal muscles and consuming energy [1]. The following applies: the more intensive the physical activity, the more energy is consumed per unit of time.
In the public health context, physical activity is defined as any bodily movement produced by skeletal muscles that results in energy expenditure [1].
The behaviour, the type and intensity of physical activity — characterised by frequency, intensity, duration, mode, and progression — is called exercise, training, or sport in different contexts. Exercise is planned, structured, and repetitive physical activity with the specific goal of improving or maintaining one or more aspects of physical fitness [1]. Here are key differences:
- Physical activity encompasses all body movements in everyday life.
- Exercise represents planned, structured activities with specific goals.
- Training involves systematic exercise for long-term adaptation.
- Sport is competitive physical activity with rules and objectives.
Energy Expenditure
Energy expenditure comprises several components:
- Basal Metabolic Rate (BMR) — energy required for essential physiological functions at rest.
- Resting Metabolic Rate (RMR) — similar to BMR but measured under less stringent conditions.
- Thermic Effect of Food (TEF) — energy required to digest, absorb, and process nutrients.
- Activity Energy Expenditure (AEE) — energy consumed during physical activity.
The key principle: Total daily energy expenditure (TDEE) = BMR + TEF + AEE + non-exercise thermogenesis (NEAT).
Estimation of Basal Metabolic Rate
Accurate estimation of BMR is a prerequisite for calculating total daily energy expenditure (TDEE) and for designing sport-specific nutrition strategies. Several prediction equations have been developed, differing in their input variables and the populations in which they were validated. The classic Harris–Benedict equations (1918, revised by Roza & Shizgal 1984) estimate BMR from body weight, height, and age separately for males and females [17, 18]. Because these equations were derived from non-athletic populations, they systematically underestimate RMR in individuals with high lean body mass. The Cunningham equation (1980) addresses this limitation by replacing anthropometric proxies with lean body mass (LBM) as the sole predictor, yielding a single sex-independent formula that better captures metabolically active tissue [19]. Building on Cunningham’s framework, Ten Haaf & Weijs (2014) confirmed its validity in recreational athletes and proposed a slightly revised coefficient set using fat-free mass (FFM) (370 + 21.6 × FFM), along with a weight-based alternative equation for situations where body composition data are unavailable [20]. For athletic populations — including strength-trained and endurance athletes — equations incorporating FFM or LBM are generally preferred over weight-based equations, as metabolically active tissue is the primary determinant of resting metabolic rate.
Although the terms lean body mass (LBM) and fat-free mass (FFM) are frequently used interchangeably in the literature, they are subtly but meaningfully distinct concepts. FFM represents everything in the body that is not fat — muscle, bone, organs, water, and connective tissue — and excludes all lipid fractions. LBM, by contrast, retains a small amount of essential fat (~3 % in males, ~12 % in females) that is physiologically indispensable (e.g., phospholipids in cell membranes, myelin sheaths, and steroid hormones) and therefore not metabolically equivalent to storage fat. Consequently, LBM ≥ FFM, with the difference typically amounting to 1–3 kg in healthy adults. This terminological inconsistency has direct relevance for BMR prediction: Cunningham (1980) formulated his equation using LBM, whereas Ten Haaf & Weijs (2014) used FFM as measured by DEXA. Because both authors refitted their respective coefficients to their own datasets, the two formulas are not term-for-term comparable. In practice, however, the resulting error when substituting FFM for LBM (or vice versa) in either equation is clinically negligible for most athletic populations, and both measures are obtained via the same instruments (DEXA, BIA, hydrostatic weighing).
The key conceptual distinctions are summarised in Table 1:
Conceptual comparison of fat-free mass (FFM) and lean body mass (LBM) in the context of BMR prediction equations.
| FFM | LBM | |
|---|---|---|
| Includes essential fat? | No | Yes (~3 % ♂ / ~12 % ♀) |
| Includes storage fat? | No | No |
| Typical value relative to the other | Lower | Higher by ~1–3 kg |
| Typical measurement methods | DEXA, BIA, hydrostatic weighing | Same methods; result is ~2–5 % higher |
| Cunningham (1980) original wording | — | Uses LBM |
| Ten Haaf & Weijs (2014) | Uses FFM | — |
Conceptual comparison of fat-free mass (FFM) and lean body mass (LBM) in the context of BMR prediction equations.
Comparison of estimation formulas of basal metabolic rate with special relevance for athletic populations (adapted from [17–20]). All values in kcal/day; LBM = lean body mass, FFM = fat-free mass, BW = body weight. Cunningham (1980) used LBM, Ten Haaf & Weijs (2014) used FFM; substituting one for the other introduces only negligible error in most athletic populations.
| Equation | Year | Formula | Input variables | Validated population |
|---|---|---|---|---|
| Harris–Benedict (original) | 1918 | ♂ BMR = 66.5 + (13.75 × kg) + (5.00 × cm) − (6.76 × age) ♀ BMR = 655.1 + (9.56 × kg) + (1.85 × cm) − (4.68 × age) | Body weight, height, age | Healthy non-athletic adults |
| Harris–Benedict (revised) | 1984 | ♂ BMR = 88.4 + (13.4 × kg) + (4.80 × cm) − (5.68 × age) ♀ BMR = 447.6 + (9.25 × kg) + (3.10 × cm) − (4.33 × age) | Body weight, height, age | Hospitalised & healthy adults |
| Cunningham | 1980 | RMR = 500 + (22 × LBM) | Lean body mass (kg) | Healthy adults; applicable to athletes |
| Ten Haaf & Weijs (FFM-based) | 2014 | REE = 370 + (21.6 × FFM) | Fat-free mass (kg) | Recreational athletes (18–35 y) |
| Ten Haaf & Weijs (weight-based) | 2014 | REE = (25.9 × BW) − 284 | Body weight (kg) | Recreational athletes (18–35 y); no body composition data required |
Comparison of estimation formulas of basal metabolic rate with special relevance for athletic populations (adapted from [17–20]). All values in kcal/day; LBM = lean body mass, FFM = fat-free mass, BW = body weight. Cunningham (1980) used LBM, Ten Haaf & Weijs (2014) used FFM; substituting one for the other introduces only negligible error in most athletic populations.
Total Energy Expenditure across the Human Life Course
Beyond resting metabolism, understanding how total energy expenditure (TEE) changes across the lifespan is fundamental for contextualising BMR within a broader metabolic framework. A landmark large-scale study published in Science (Pontzer et al., 2021) [21] demonstrated that TEE is strongly determined by fat-free mass (muscle mass) and follows a distinct age-related trajectory. Using doubly labelled water data from over 6,400 individuals across 29 countries (aged 8 days to 95 years), the authors identified four distinct metabolic phases across the human lifespan [22]:
- Infancy and childhood (0–20 years): TEE adjusted for FFM rises sharply during infancy, peaks in early childhood (~1 year of age at ~50 % above adult levels), then progressively declines through adolescence.
- Adulthood plateau (20–60 years): A stable phase in which TEE adjusted for FFM remains essentially constant, independent of sex or reproductive status. Notably, sex differences in TEE disappear once FFM is accounted for — females do not have inherently lower metabolic rates than males when lean tissue mass is controlled.
- Late-life decline (> 60 years): A second declining phase begins around age 60, independent of changes in body composition or physical activity levels, reflecting a genuine reduction in tissue-level metabolic rate.
- Clinical relevance: The marked rise in incidence of chronic disease from late middle age closely aligns with the shift in TEE and progressive loss of adiposity, suggesting that metabolism may be a driver in ageing biology rather than merely a passive correlate [21, 22].
These findings have direct implications for BMR prediction in exercise and sports science contexts: equations validated in young athletic adults (e.g. Ten Haaf & Weijs, 2014) may systematically overestimate REE in masters athletes or older recreational exercisers, for whom age-related reductions in both FFM and tissue-specific metabolic rates must be considered.
- Pontzer et al. (2021) — Daily energy expenditure through the human life course (Science)
- Rhoads & Anderson (2021) — Taking the long view on metabolism (Science)
Online Calculators
The following tools allow students and practitioners to apply BMR/RMR prediction equations interactively without manual calculation. The USDA Dietary Reference Intakes (DRI) Calculator provides evidence-based energy and nutrient estimates for a wide range of age groups and activity levels, drawing on the equations recommended by the National Academies of Medicine. The Cunningham RMR Calculator by Peter Bond implements the Cunningham (1980) equation directly, requiring only a fat-free mass estimate — making it particularly useful for athletes and individuals with known body composition data.
Metabolic Strain and Physiological Responses
Physical activity exerts a metabolic strain on the organism. The physiological strain depends on:
- Type of activity — aerobic vs. anaerobic, resistance vs. endurance.
- Intensity — measured as % of V̇O₂max or % of maximal heart rate.
- Duration — single bout vs. cumulative effects.
- Frequency — how often the activity is performed.
- Individual factors — age, fitness level, health status.
The organism responds to metabolic strain through acute physiological adjustments (heart rate increase, breathing rate increase) and chronic adaptations (mitochondrial biogenesis, improved capillary density).
2 Short-Term Balancing of Homeostasis
Concept of Homeostasis
Homeostasis refers to the dynamic equilibrium of the internal environment, maintained through regulatory mechanisms that counteract disturbances. Physical activity is a significant disturbance to homeostasis, triggering rapid regulatory responses.
Homeostasis refers to the dynamic equilibrium of the internal environment, maintained through regulatory mechanisms that counteract disturbances. Physical activity is a significant disturbance to homeostasis, triggering rapid regulatory responses.
Acute Responses to Exercise
Acute physical stress, for example through physical activity, leads to a disruption of homeostasis. The disruption of homeostasis is rebalanced by physiological mechanisms and returns to a state of rest. For example, physical exertion leads to increased breathing in order to absorb more oxygen. In order for the oxygen in the blood to be transported to the muscles, the blood circulation must be increased. In order for the blood circulation to increase, the duration of the heartbeats must be shortened with a simultaneous increase in the stroke volume. In order to increase ventilation, the depth of the breath and the respiratory rate must be increased. The increase in circulation and ventilation leads to increased oxygen intake in the organism. Ventilation and duration of heart beats are typical physiological parameters to describe the functions of the respiratory and cardiovascular system
When the organism engages in physical activity, multiple physiological systems are activated simultaneously:
Cardiovascular Response
- Heart rate increases to deliver more oxygen and nutrients to working muscles.
- Stroke volume increases — the heart pumps more blood per beat.
- Blood pressure rises — systolic increases more than diastolic.
- Blood flow redistribution — 20–25 % of cardiac output at rest goes to muscles; during exercise, this increases to 85–90 %.
Example for acute disturbance of the homeostasis by acute physical stress. Heart rate and ventilation increase during exercise and return after the end of the exercise. Light blue lines: physical rest before exercise, red lines: incremental graded maximal cycle ergometer exercise, dark blue lines: physical rest after the end of exercise.
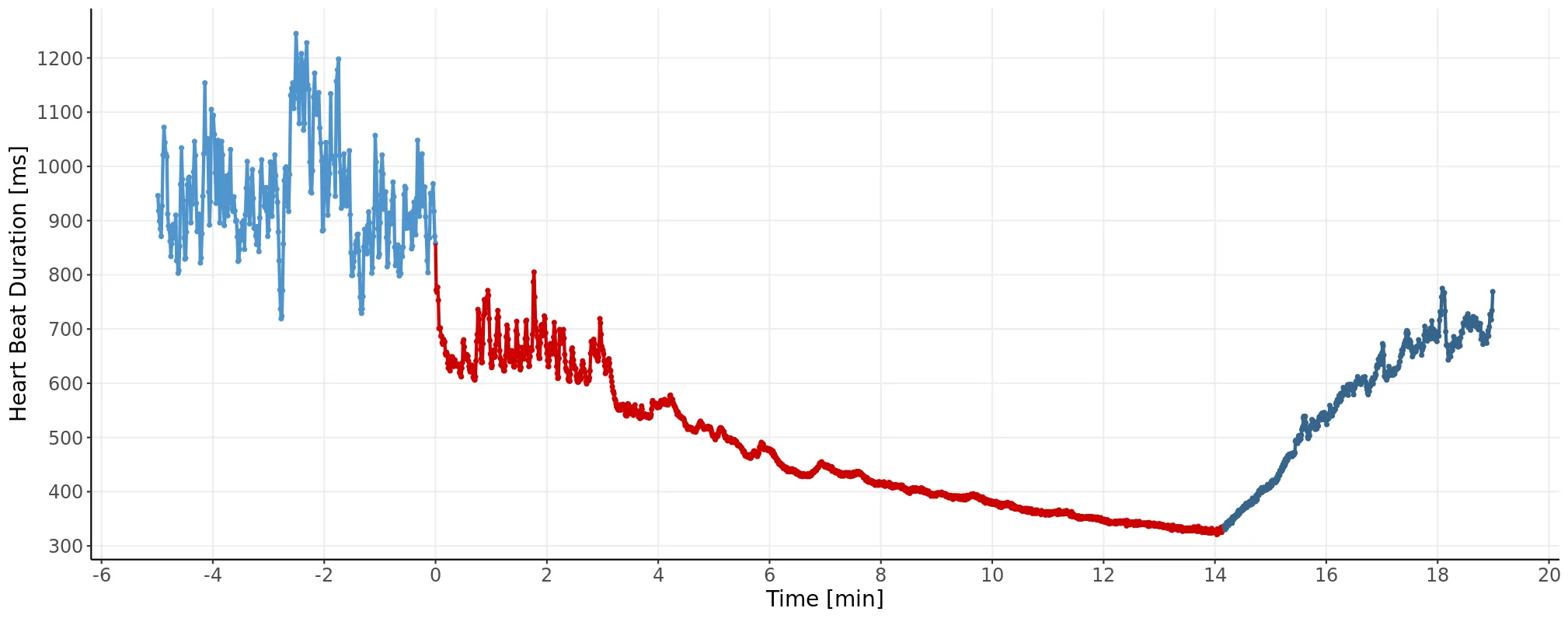

Example for acute disturbance of the homeostasis by acute physical stress. Heart rate and ventilation increase during exercise and return after the end of the exercise. Light blue lines: physical rest before exercise, red lines: incremental graded maximal cycle ergometer exercise, dark blue lines: physical rest after the end of exercise.
Respiratory Response
- Breathing frequency increases to enhance gas exchange.
- Tidal volume increases — greater volume of air per breath.
- Minute ventilation (V̇E) increases proportionally to exercise intensity.
- V̇O₂ increases — more oxygen is extracted from inhaled air.
Metabolic Response
- ATP demand increases — muscle contractions require rapid ATP regeneration.
- Substrate utilization shifts — at low intensities, fats dominate; at high intensities, carbohydrates predominate.
- Lactate production increases — anaerobic metabolism becomes significant above the anaerobic threshold.
- Hormone secretion increases — catecholamines, cortisol, and glucagon mobilize energy substrates.
Temperature Regulation
- Core body temperature rises due to metabolic heat production.
- Sweating increases — the primary mechanism for heat dissipation during exercise.
- Skin blood flow increases — facilitates heat loss to the environment.
Recovery and Return to Baseline
Upon cessation of exercise, the organism enters a recovery phase characterized by:
- Gradual reduction in heart rate and breathing rate — occurs in stages (fast and slow phases).
- Restoration of muscle glycogen — aided by insulin sensitivity and GLUT4 translocation.
- Lactate clearance — lactate is oxidized in slow-twitch fibers and the liver.
- Hormonal normalization — stress hormones return to baseline; anabolic hormones increase.
- EPOC (Excess Post-Exercise Oxygen Consumption) — elevated metabolic rate persisting after exercise, fueling recovery processes.
Practical insight: The recovery phase is critical. Regular physical activity improves the efficiency of these regulatory mechanisms, reducing the time required to return to baseline and enhancing overall homeostatic stability.
3 Homeostasis and Hormesis
From Homeostatic Regulation to Hormetic Adaptation
The acute physiological responses described in Section 2 restore internal equilibrium through negative feedback — a process canonically attributed to Claude Bernard and Walter Cannon [2]. However, the observation that repeated exercise bouts lead not merely to restoration of the original baseline but to a higher functional set-point demands a second explanatory framework: hormesis [3, 4].
Hormesis describes the biphasic dose-response relationship in which low-to-moderate doses of a stressor produce beneficial effects opposite to those observed at high doses [3]. In exercise physiology, this means that the very inflammatory mediators serving as homeostatic error signals — IL-6, reactive oxygen species (ROS), NF-κB — simultaneously function as dose-dependent adaptive triggers when present at appropriate magnitudes and durations [4].
More formally, “hormesis refers to adaptive responses of biological systems to moderate environmental or self-imposed challenges through which the system improves its functionality and/or tolerance to more severe challenges. In other words, hormesis is a coordinated response of cells and organisms to an imposed or intrinsically generated challenge that involves multiple integrative signal-transduction processes, each of which is quantitatively hormetic, to coordinate a final holistic response” [15].
Hormetic Stress Response
Skeletal muscle and the broader physiological system perpetually encounter intrinsic mechanical and metabolic challenges imposed by physical activity. To cope with exercise-induced stressors — including mechanical loading, metabolic perturbation, oxidative stress, hypoxia, muscle damage, and thermal stress arising from sustained exertion — living organisms have evolved adaptive, protective training responses. At the molecular, cellular, and whole-organism levels, these responses share common regulatory features collectively termed ‘exercise stress’ and rely on evolutionarily conserved, exercise-responsive transcriptional networks [16]. The pattern of exercise-induced adaptations is dictated not only by the specific type of training stimulus (e.g., resistance, endurance, or concurrent exercise) but also by its intensity, frequency, and duration — variables central to exercise programming. Each of these factors, alone or in combination, can transiently disrupt physiological homeostasis and impair functional capacity. Sub-maximal training loads, however, elicit beneficial adaptive responses — including muscle hypertrophy, mitochondrial biogenesis, and improved cardiovascular function — that attenuate the physiological cost of subsequent bouts of the same or related exercise stress. This dose-dependent, biphasic adaptive property is known as ‘hormesis’ [15, 16]. A hallmark of exercise-induced hormesis is that the adaptive response to a given exercise stressor can extend cross-protective effects against future, and apparently unrelated, forms of physiological stress. The architecture of the exercise-responsive transcriptional network, whereby distinct modes of training regulate overlapping profiles of effector genes — including those encoding heat shock proteins, pro- and anti-inflammatory immune responses, antioxidant enzymes, and angiogenic factors — provides a compelling mechanistic explanation for this phenomenon [16].
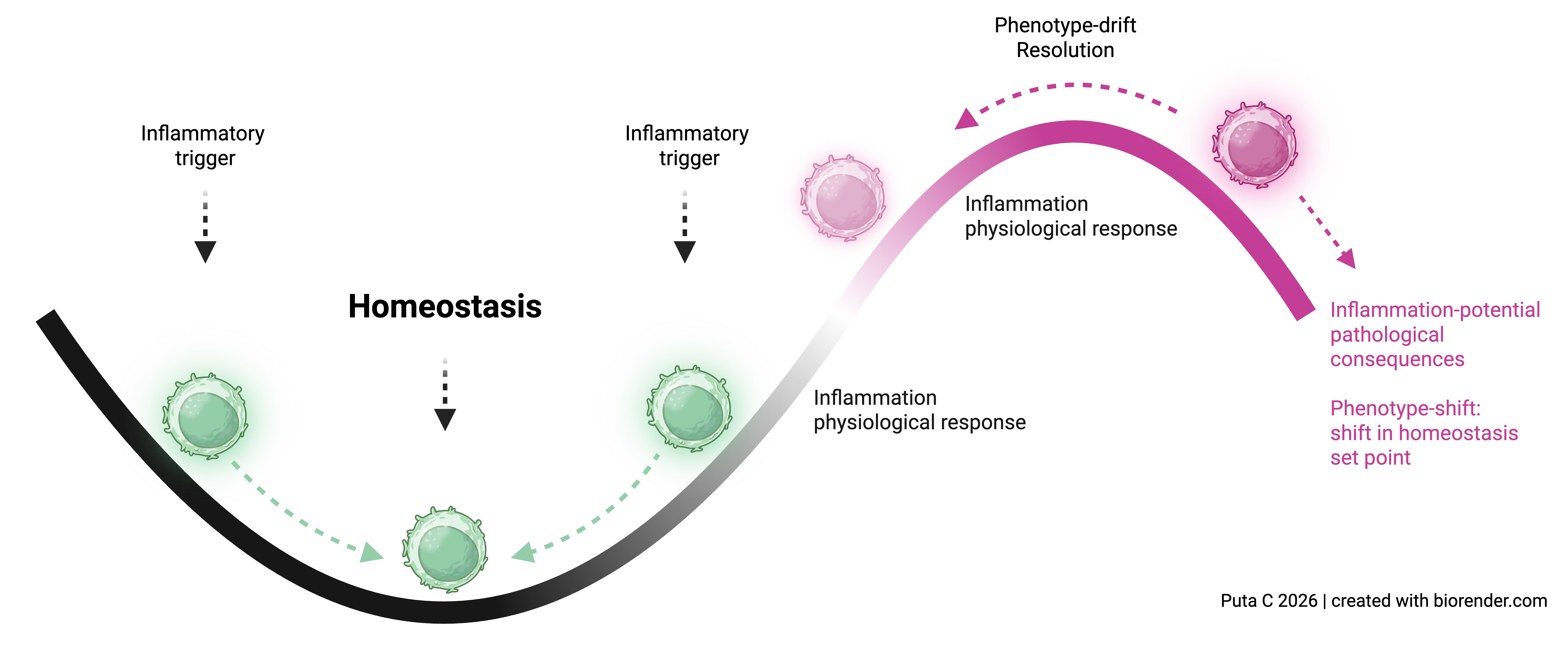
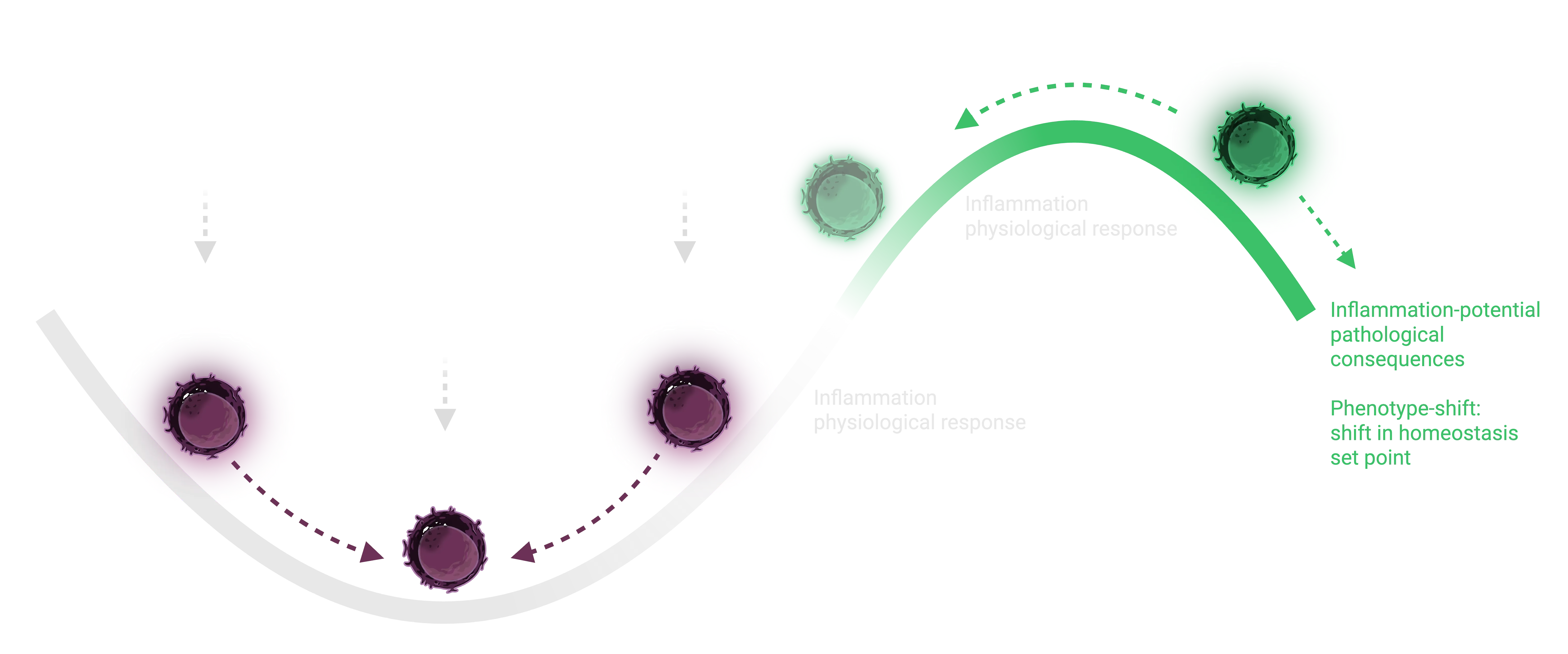
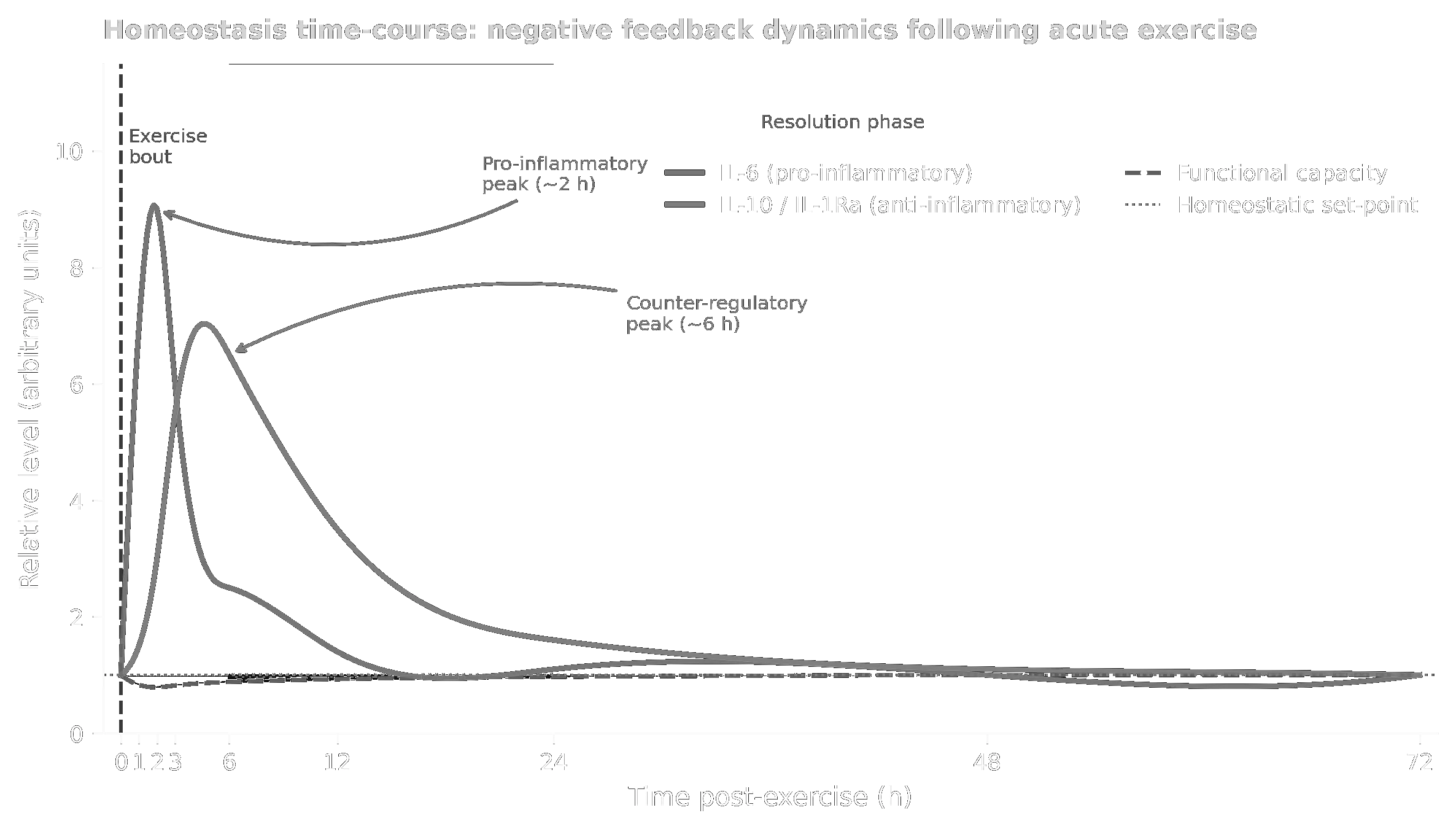
Homeostasis time-course: the IL-6 peak, delayed IL-10/IL-1Ra counter-response, functional capacity dip, and the set-point reference line, with annotated phase zones.
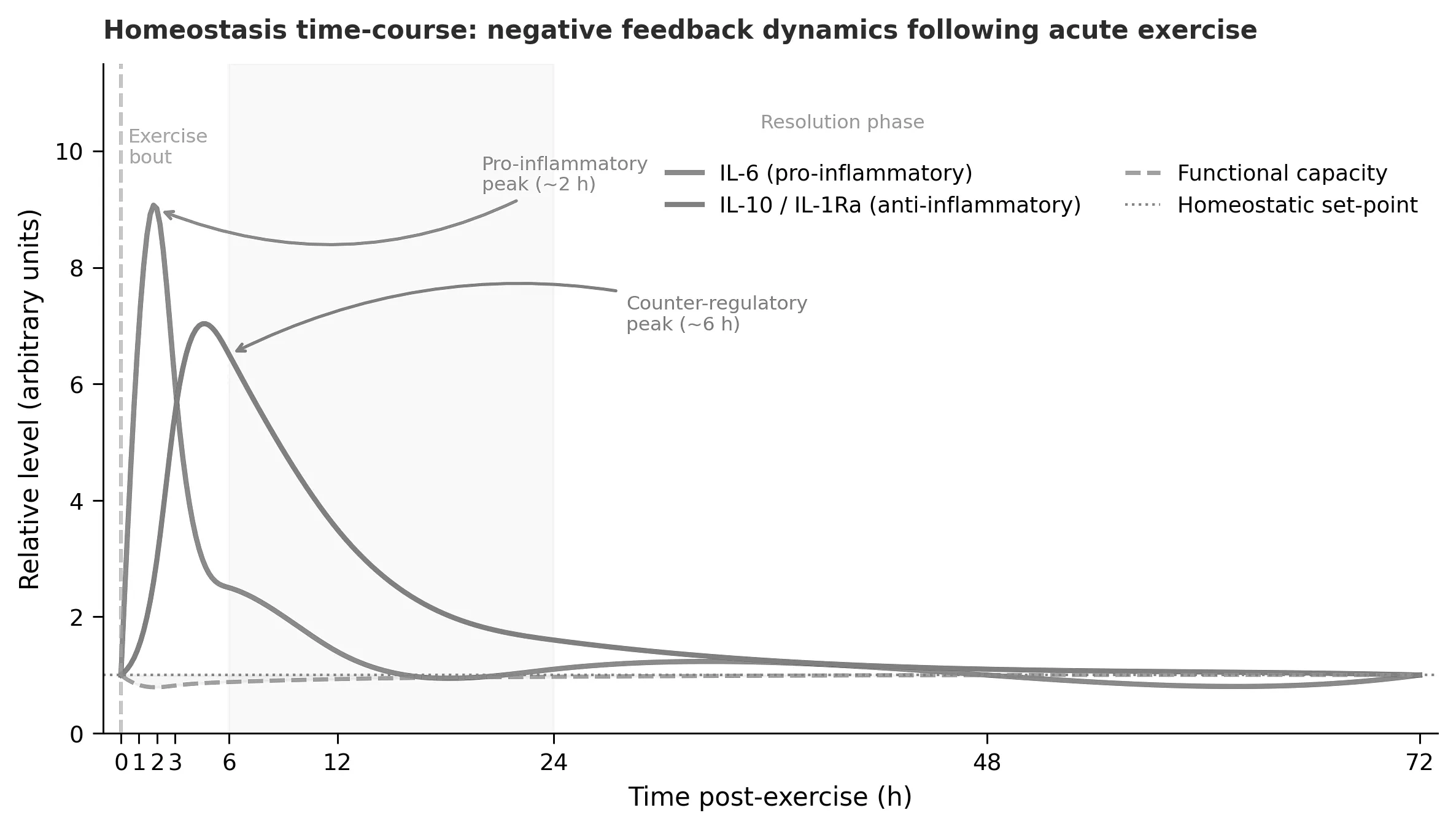
Homeostasis time-course: the IL-6 peak, delayed IL-10/IL-1Ra counter-response, functional capacity dip, and the set-point reference line, with annotated phase zones.
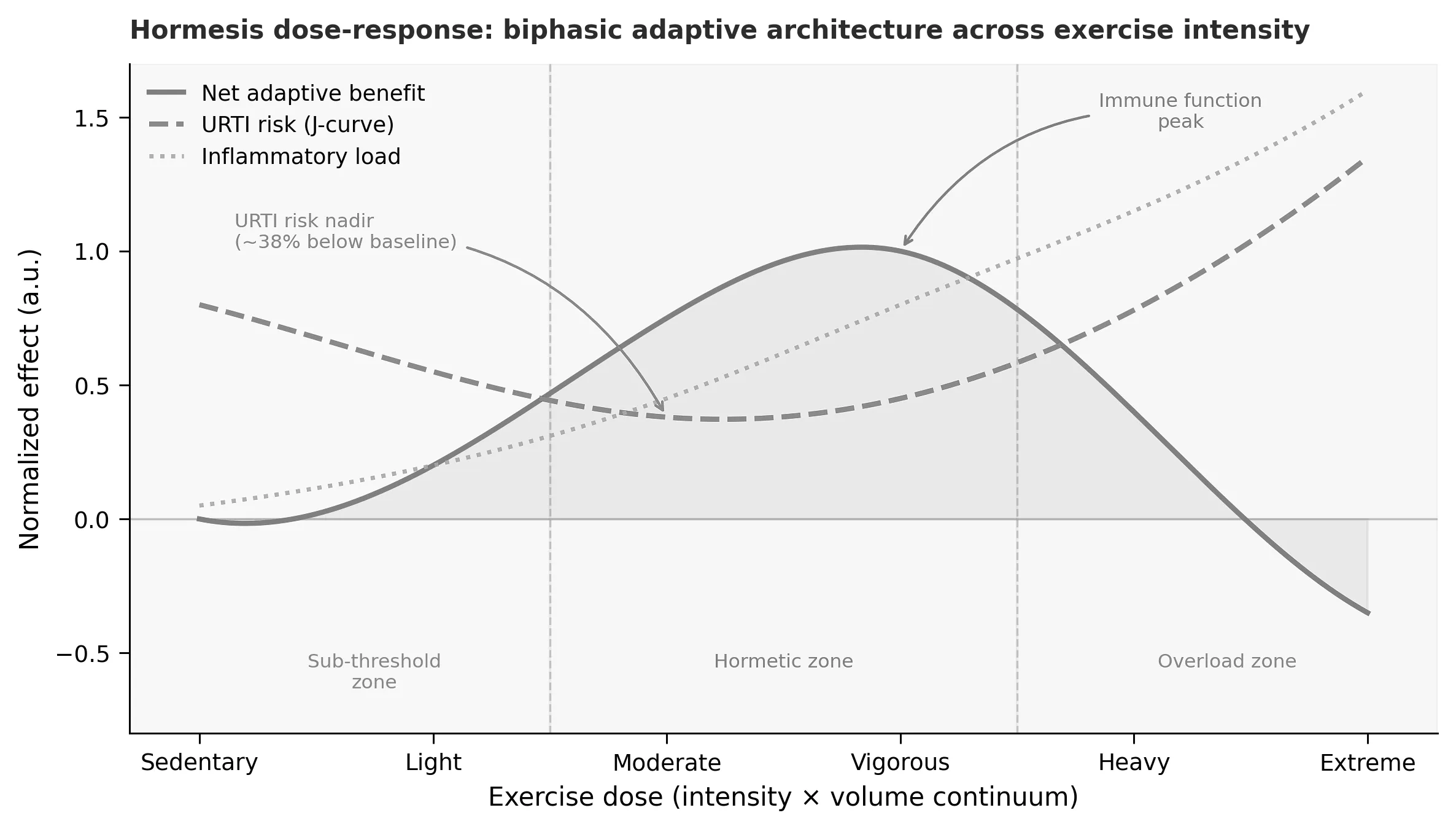
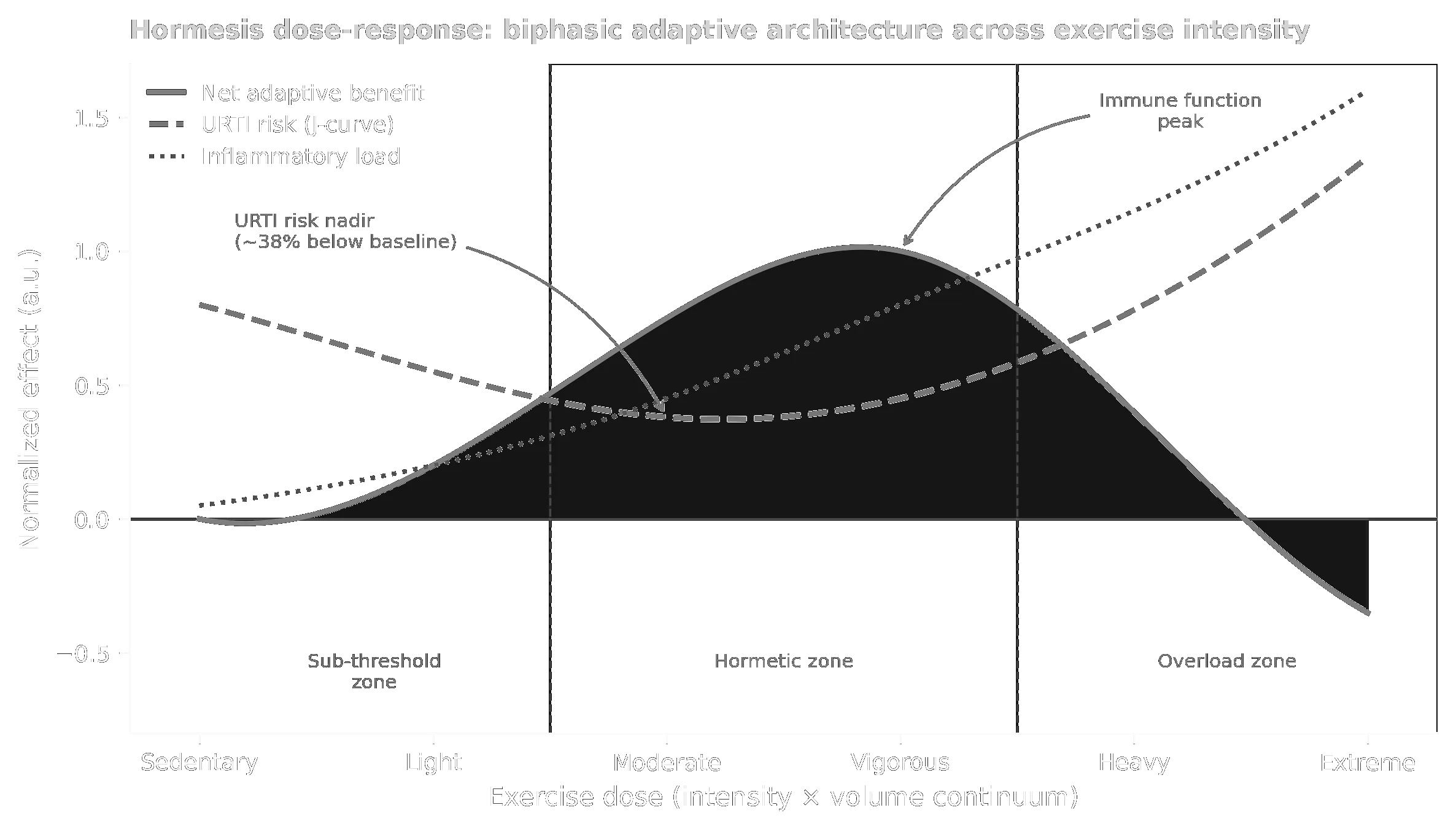
Hormesis dose-response: the full J-curve (URTI risk), bell-shaped adaptive benefit, and monotonically rising inflammatory load, with the three dose zones (sub-threshold / hormetic / overload) shaded.
Hormesis dose-response: the full J-curve (URTI risk), bell-shaped adaptive benefit, and monotonically rising inflammatory load, with the three dose zones (sub-threshold / hormetic / overload) shaded.
The Dual Identity of Inflammatory Mediators
The juxtaposition of homeostasis and hormesis reveals that the same molecular entities serve different functional roles depending on dose and context [5]:
- Interleukin-6 (IL-6) functions as a homeostatic error signal communicating perturbation magnitude to the hypothalamus and liver, yet simultaneously acts as a myokine with insulin-sensitising, lipolytic, and anti-inflammatory properties that drive long-term adaptation [6].
- Reactive oxygen species (ROS) act as homeostatic damage markers activating NF-κB-driven repair programs at low concentrations, while simultaneously triggering Nrf2-mediated antioxidant upregulation through a hormetic pathway [7].
- NF-κB activates both pro-inflammatory gene targets (TNF-α, IL-1β, COX-2) and protective ones (antioxidant enzymes, anti-apoptotic factors), with the net outcome determined by the intensity and duration of its activation [5].
Molecular Mediators of the Hormetic Response
At the molecular level, the hormetic response to exercise is mediated by overlapping stress-response pathways [3, 4]:
- Nrf2 (nuclear factor erythroid 2-related factor 2): activated by exercise-generated ROS; drives the transcription of antioxidant enzymes (SOD, catalase, glutathione peroxidase) and phase II detoxification enzymes.
- PGC-1α (peroxisome proliferator-activated receptor gamma coactivator 1-alpha): activated by AMP/ATP ratio, intracellular calcium, and ROS; orchestrates mitochondrial biogenesis, fibre type transition, and VEGF-driven angiogenesis.
- Heat-shock proteins (HSPs), particularly HSP70 and HSP90: upregulated in response to thermal and oxidative stress; act as molecular chaperones protecting structural and contractile proteins.
- Autophagy induction: exercise activates AMPK-mediated autophagy, clearing dysfunctional organelles and misfolded proteins, contributing to cellular quality control.
A crucial insight is that complete suppression of inflammation — for example through NSAIDs or antioxidants immediately post-exercise — may blunt the adaptive signal and attenuate training-induced gains [8, 9].
Biphasic Dose-Response and the J-Curve of Immune Function
The hormesis framework organises the exercise dose-response into three operationally distinct zones [5, 10]:
- Sub-threshold zone (sedentary to light activity): insufficient stimulus for meaningful adaptive programming.
- Hormetic zone (moderate to vigorous exercise): net adaptive benefit peaks; URTI risk falls approximately 38 % below population average [10]; Nrf2 and PGC-1α pathways are maximally activated.
- Overload zone (extreme training load): inflammatory load overwhelms adaptive reserves; immune suppression ensues consistent with the open-window hypothesis [10, 11].
The J-curve of upper respiratory tract infection (URTI) risk across the exercise intensity spectrum, first articulated by Nieman [10], is the most widely cited empirical anchor for the hormetic dose-response in exercise immunology. At the moderate exercise level, URTI risk reaches its nadir; at the heavy-to-extreme transition, URTI risk exceeds the sedentary baseline, marking the operational equivalent of the hormetic toxicity threshold.
Complementary Temporal Scales
Homeostasis and hormesis are not competing theories but complementary descriptions of the same biology at different temporal scales [5]:
- In the acute window (0–24 h post-exercise), the homeostatic frame predominates: the organism’s priority is to restore internal equilibrium through negative feedback.
- In the sub-acute and chronic adaptation window (24 h to multiple training cycles), the hormetic frame becomes operative: if the inflammatory signal was of appropriate magnitude and the resolution phase was complete, molecular memory — in the form of elevated Nrf2 target gene expression, increased mitochondrial density, and epigenetic modification of stress-response promoters — shifts the set-point upward (supercompensation).
Mechanistic contrast between homeostasis and hormesis frameworks applied to exercise-induced inflammation (adapted from [5]).
| Dimension | Homeostasis framework | Hormesis framework |
|---|---|---|
| Primary signal role of IL-6/ROS | Error signal (perturbation magnitude) | Adaptive stimulus (dose-dependent trigger) |
| Feedback direction | Negative (corrective) | Forward at low dose; negative at overload |
| Set-point outcome | Preserved at baseline | Elevated (supercompensation) |
| Dose-response shape | Linear / monotonic resolution | Biphasic / inverted-U |
| Inflammation framing | Perturbation to be resolved | Necessary adaptive trigger |
| Key regulatory node | IL-10 axis, HPA cortisol | Nrf2, PGC-1α, HSPs, autophagy |
| Optimal treatment strategy | Anti-inflammatory resolution support | Preserve signal; avoid premature blunting |
| Failure mode | Unresolved chronic inflammation | Overtraining / immunosuppression |
Mechanistic contrast between homeostasis and hormesis frameworks applied to exercise-induced inflammation (adapted from [5]).
Pathological Contexts: ME/CFS, Long COVID, and Post-Exertional Malaise
In populations with myalgic encephalomyelitis/chronic fatigue syndrome (ME/CFS) and Long COVID, post-exertional malaise (PEM) represents a pathological exaggeration of the post-exercise inflammatory state [12, 13]. Within the dual-framework model, PEM can be conceptualised as a combination of two discrete abnormalities [5]:
- Failure of homeostatic resolution: the counter-regulatory response (IL-10, IL-1Ra) is either insufficient, delayed, or overridden by persistent upstream activation, leaving the inflammatory perturbation unresolved beyond 24–48 h.
- Right-shift or inversion of the hormetic dose-response curve: the threshold between the sub-threshold and overload zones narrows critically, such that exercise doses producing adaptive benefits in healthy individuals fall within or above the overload zone for the affected individual.
This model provides a theoretical basis for the observation that graded exercise therapy (GET) — predicated on the homeostatic assumption that graduated perturbations will lead to adaptive set-point elevation — is not only ineffective but actively harmful in ME/CFS, because the hormetic adaptive machinery is unavailable or compromised [5, 12, 13].
Practical insight: Homeostasis governs the immediate inflammatory resolution following exercise, while hormesis explains the long-term adaptive gains. Recognising their complementary nature is essential for optimal exercise prescription — particularly in clinical populations where resolution capacity may be impaired and the hormetic dose-response curve may be critically altered.
4 State of Sleep and Wakefulness
Sleep Architecture and Physiology
Sleep is a vital physiological state characterized by reduced responsiveness to external stimuli and reversibility. It consists of two main types:
Non-REM (NREM) Sleep
- Stage 1 (Light sleep): Transition from wakefulness; muscle tone decreases; brain waves slow.
- Stage 2 (Intermediate sleep): Further slowing of brain waves; characterized by sleep spindles and K-complexes.
- Stage 3 (Deep sleep/Slow-wave sleep): Highest threshold for arousal; greatest brain wave slowing; major restorative processes occur.
REM Sleep (Rapid Eye Movement Sleep)
- Characterized by rapid eye movements, muscle atonia, and vivid dreams.
- Brain activity resembles wakefulness, but voluntary movement is inhibited.
- Occupies ~20–25 % of total sleep time in adults.
Sleep Cycles and Duration
A complete sleep cycle lasts approximately 90 minutes and progresses through stages 1–3 of NREM followed by REM sleep. Most restorative sleep occurs during stages 3 (deep sleep) and REM phases. Adults require 7–9 hours of sleep per night for optimal physiological function.
Physiological Functions of Sleep
Sleep serves multiple critical functions:
- Physical restoration — tissue repair, protein synthesis, growth hormone secretion.
- Metabolic regulation — glucose homeostasis, insulin sensitivity, lipid metabolism.
- Immune function — T-cell proliferation, cytokine production, immune memory consolidation.
- Cognitive consolidation — memory consolidation (both declarative and procedural).
- Cerebral clearance — removal of metabolic waste products via the glymphatic system.
- Thermoregulation — core body temperature decreases during sleep.
Relationship Between Exercise and Sleep
Physical activity promotes sleep quality through multiple mechanisms:
- Increased sleep pressure — physical activity depletes energy substrates and increases adenosine, promoting sleep.
- Enhanced thermoregulation — exercise-induced increase in core body temperature followed by a rapid drop facilitates sleep onset.
- Stress reduction — regular physical activity reduces cortisol levels and psychological stress.
- Improved circadian alignment — morning exercise synchronizes the circadian rhythm, facilitating sleep at appropriate times.
Sleep deprivation impairs exercise performance and recovery:
- Reduced strength and power output.
- Increased injury risk — impaired neuromuscular control.
- Blunted training adaptations — reduced mitochondrial biogenesis and angiogenesis.
- Immune suppression — increased susceptibility to infections.
- Metabolic dysregulation — increased carbohydrate cravings and reduced insulin sensitivity.
Practical insight: A bidirectional relationship exists between exercise and sleep. Regular physical activity improves sleep quality, and adequate sleep enhances exercise performance and training adaptations. Prioritizing both is essential for optimal health outcomes.
References
- [1] Caspersen CJ, Powell KE, Christenson GM. Physical activity, exercise, and physical fitness: definitions and distinctions for health-related research. Public Health Reports. 1985;100(2):126–131. ISSN 0033-3549.
- [2] Cannon WB. The Wisdom of the Body. W. W. Norton & Company; 1932.
- [3] Calabrese EJ, Baldwin LA. Defining hormesis. Human & Experimental Toxicology. 2002;21(2):91–97.
- [4] Calabrese EJ, Mattson MP. How does hormesis impact biology, toxicology and medicine? npj Aging and Mechanisms of Disease. 2017;3:13.
- [5] Puta C, Gabriel H. Homeostasis and hormesis as complementary frameworks for exercise-induced inflammation: a conceptual simulation analysis. Friedrich-Schiller-Universität Jena, Institute for Sports Science; 2025.
- [6] Pedersen BK, Febbraio MA. Muscle as an endocrine organ: focus on muscle-derived interleukin-6. Physiological Reviews. 2008;88(4):1379–1406.
- [7] Ristow M, Zarse K, Oberbach A, et al. Antioxidants prevent health-promoting effects of physical exercise in humans. Proceedings of the National Academy of Sciences. 2009;106(21):8665–8670.
- [8] Paulsen G, Cumming KT, Holden G, et al. Vitamin C and E supplementation hampers cellular adaptation to endurance training in humans. Journal of Physiology. 2014;592(8):1887–1901.
- [9] Selye H. The general adaptation syndrome and the diseases of adaptation. Journal of Clinical Endocrinology and Metabolism. 1946;6(2):117–230.
- [10] Nieman DC. Exercise, infection, and immunity. International Journal of Sports Medicine. 1994;15(S3):S131–S141.
- [11] Nieman DC, Wentz LM. The compelling link between physical activity and the body’s defense system. Journal of Sport and Health Science. 2019;8(3):201–217.
- [12] Carruthers BM, van de Sande MI, De Meirleir KL, et al. Myalgic encephalomyelitis: International consensus criteria. Journal of Internal Medicine. 2011;270(4):327–338.
- [13] Komaroff AL, Lipkin WI. Insights from myalgic encephalomyelitis/chronic fatigue syndrome may help unravel the pathogenesis of post-acute COVID-19 syndrome. Trends in Molecular Medicine. 2021;27(9):895–906.
- [14] Gleeson M, Bishop NC, Stensel DJ, Lindley MR, Mastana SS, Nimmo MA. The anti-inflammatory effects of exercise: mechanisms and implications for the prevention and treatment of disease. Nature Reviews Immunology. 2011;11(9):607–615.
- [15] Calabrese EJ, Mattson MP. How does hormesis impact biology, toxicology, and medicine? npj Aging and Mechanisms of Disease. 2017;3:13. doi:10.1038/s41514-017-0013-z.
- [16] Bauer M, Ermolaeva M, Singer M, Wetzker R, Soares MP. Hormesis as an adaptive response to infection. Trends in Molecular Medicine. 2024;30(7):633–642. doi:10.1016/j.molmed.2024.04.012.
- [17] Harris JA, Benedict FG. A biometric study of human basal metabolism. Proceedings of the National Academy of Sciences. 1918;4(12):370–373. doi:10.1073/pnas.4.12.370.
- [18] Roza AM, Shizgal HM. The Harris Benedict equation reevaluated: resting energy requirements and the body cell mass. The American Journal of Clinical Nutrition. 1984;40(1):168–182. doi:10.1093/ajcn/40.1.168.
- [19] Cunningham JJ. A reanalysis of the factors influencing basal metabolic rate in normal adults. The American Journal of Clinical Nutrition. 1980;33(11):2372–2374. doi:10.1093/ajcn/33.11.2372.
- [20] Ten Haaf T, Weijs PJM. Resting energy expenditure prediction in recreational athletes of 18–35 years: confirmation of Cunningham equation and an improved weight-based alternative. PLOS ONE. 2014;9(9):e108460. doi:10.1371/journal.pone.0108460.
- [21] Pontzer H, Yamada Y, Sagayama H, et al. Daily energy expenditure through the human life course. Science. 2021;373(6556):808–812. doi:10.1126/science.abe5017.
- [22] Rhoads TW, Anderson RM. Taking the long view on metabolism. Science. 2021 Aug 13;373(6556):738–739. doi:10.1126/science.abl4537. PMID: 34385381.
One-Minute-Paper Topics
A One-Minute-Paper (OMP) is a short, focused prompt that students answer in ~60 seconds at the end of a session to consolidate learning, surface misconceptions, and provide formative feedback. When answering, be concise, specific, and use terminology from today’s session.
- Distinguish “physical activity” from “exercise” using one concrete example for each.
- Define energy expenditure in your own words and name two factors that modulate it acutely.
- Explain why metabolic strain during exercise is best described as a regulated rather than a passive process.
- Describe one cardiovascular response that helps maintain homeostasis during moderate exercise.
- Describe one respiratory adjustment that occurs within seconds of starting exercise and explain its purpose.
- Why does core temperature rise during exercise even though thermoregulatory mechanisms are activated?
- Define homeostasis using the principle of negative feedback and give one exercise-related example.
- Define hormesis and explain why it is described as a biphasic dose-response relationship.
- Contrast homeostasis and hormesis: which framework better describes long-term training adaptation, and why?
- Why can the same inflammatory signal be beneficial in a healthy athlete but harmful in a patient with ME/CFS or Long COVID?
- Give one example of an exercise-induced inflammatory response that is adaptive and one that is maladaptive.
- Explain how the concept of “allostatic load” might bridge homeostasis and hormesis.
- Outline the main stages of sleep architecture and identify which stage is most associated with physical recovery.
- What distinguishes NREM from REM sleep at a physiological level?
- Describe the bidirectional relationship between exercise and sleep quality with one mechanism in each direction.
- Why might evening high-intensity exercise impair sleep onset in some individuals?
- How could chronic sleep restriction undermine the hormetic benefits of training?
- Identify one measurable physiological marker you could use to monitor recovery from exercise stress.
- Which concept from today’s lecture was most surprising or counter-intuitive to you, and why?
- What single question about homeostasis, hormesis, or sleep would you most like answered in the next lecture?